$50 Billion Rural Health Program Awards Released; States Question Allocation Schedule
The Centers for Medicare & Medicaid Services issued final awards Dec. 29 under a five-year, $50 billion Rural Health Transformation Program aimed at shoring up care in America’s rural communities. While the funding offers a rare federal investment in workforce, infrastructure and telehealth, the apportionment schedule and design have left some state leaders and rural advocates worrying about equity, timing and accountability.

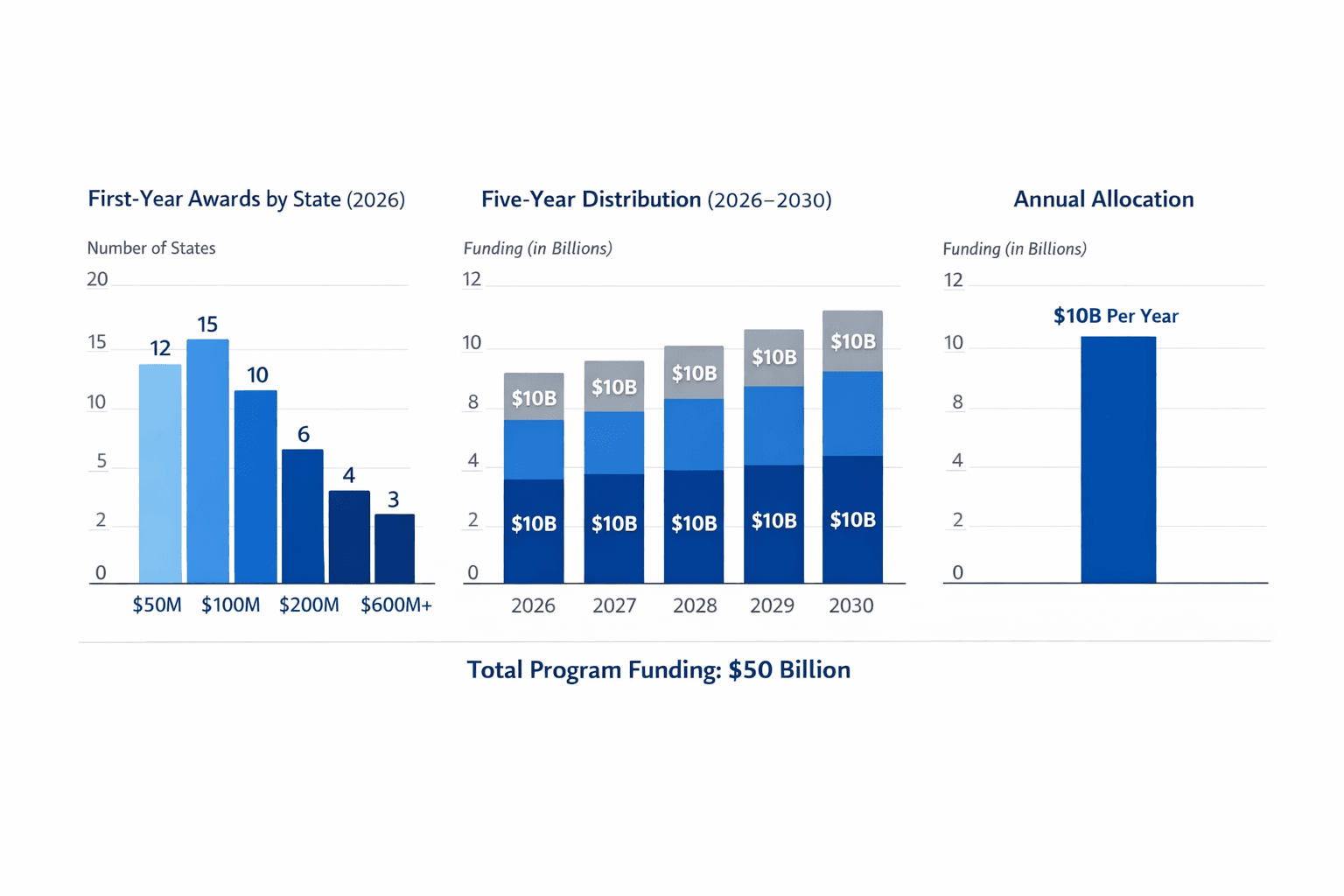
The Centers for Medicare & Medicaid Services issued final awards on Dec. 29, 2025, under the Rural Health Transformation Program, a five-year federal initiative that will apportion $10 billion annually from 2026 through 2030 to bolster care in rural areas. Created by Public Law 119-21 and later expanded by additional legislation, the $50 billion program is being overseen by a new Office of Rural Health Transformation established by the HHS Secretary within the Center for Medicaid and CHIP Services on Dec. 18, 2025.
CMS distributed first-year awards that average roughly $200 million per state, with individual state allocations ranging from about $147 million to $281 million. Texas and Alaska received the largest first-year allotments. The full five-year allotment will be distributed to approved states over the 2026–2030 period, with $10 billion available for obligation each fiscal year.
The program’s stated objectives are broad: increasing access to care in rural communities, strengthening the rural clinical workforce, modernizing infrastructure and technology including telehealth, advancing innovative payment and care models, and promoting regional collaboration to improve sustainability and patient outcomes. CMS has charged the Office of Rural Health Transformation with developing application criteria, distributing funds, providing policy guidance, monitoring progress, conducting training, and ensuring program accountability.
States competed for awards through an application window that ran from Sept. 15 to Nov. 5, 2025. CMS used a two-tier review process that guaranteed an equal baseline payment to applicants and then applied merit-based scoring in a second tier, with scores reviewed by rural health experts. States must submit annual updates on progress, but CMS reporting indicates that funding is not explicitly contingent on performance metrics, a design feature that has drawn scrutiny from policy analysts and some state officials.
Concerns center on distribution mechanics and the potential for uneven impact. Rural health leaders and state administrators have raised questions about how apportionments align with underlying need, including disparities in workforce shortages, hospital closures and broadband access that vary widely across counties and states. The phased, annual apportionment of funds could complicate planning for immediate infrastructure projects or rapid workforce investments in communities facing urgent service losses.
The program also incorporates policy expectations for states as part of some applications. States may be required to implement or maintain policy actions such as licensure compacts or Medicaid reforms tailored to their plans, though specific conditions differ by state application and CMS guidance. Hospital groups and rural providers have urged that funds be prioritized for workforce recruitment and retention, upgraded facilities, interoperable telehealth platforms and clear reporting so investments can be tracked separately on Medicare cost reports.
Advocates emphasize the potential for meaningful change if federal funds are paired with state policy reforms that address structural barriers to rural care. Critics warn that without stronger performance accountability and clearer tie-ins to Medicaid policy, the program risks widening gaps between states that can rapidly deploy funds and those hampered by administrative capacity or preexisting policy constraints.
CMS has published apportionment materials detailing state allocations and application requirements. As states begin to receive funds and submit implementation plans, follow-up reporting will focus on how investments translate into on-the-ground gains for rural residents, whether the funding narrows long-standing disparities, and how federal oversight enforces equity and measurable outcomes.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?