ADHD is linked to chronic pain, researchers probe why
ADHD and chronic pain often overlap, and new research suggests shared biology may be hiding in plain sight for patients and clinicians.

ADHD is often treated as a discrete neurodevelopmental diagnosis, but the overlap with chronic pain points to a broader clinical reality. Chronic pain affects millions of adults in the United States, and researchers are increasingly finding that people with ADHD show up in pain clinics, psychiatric settings, and genetic studies at higher-than-expected rates.
A common condition with a hidden companion
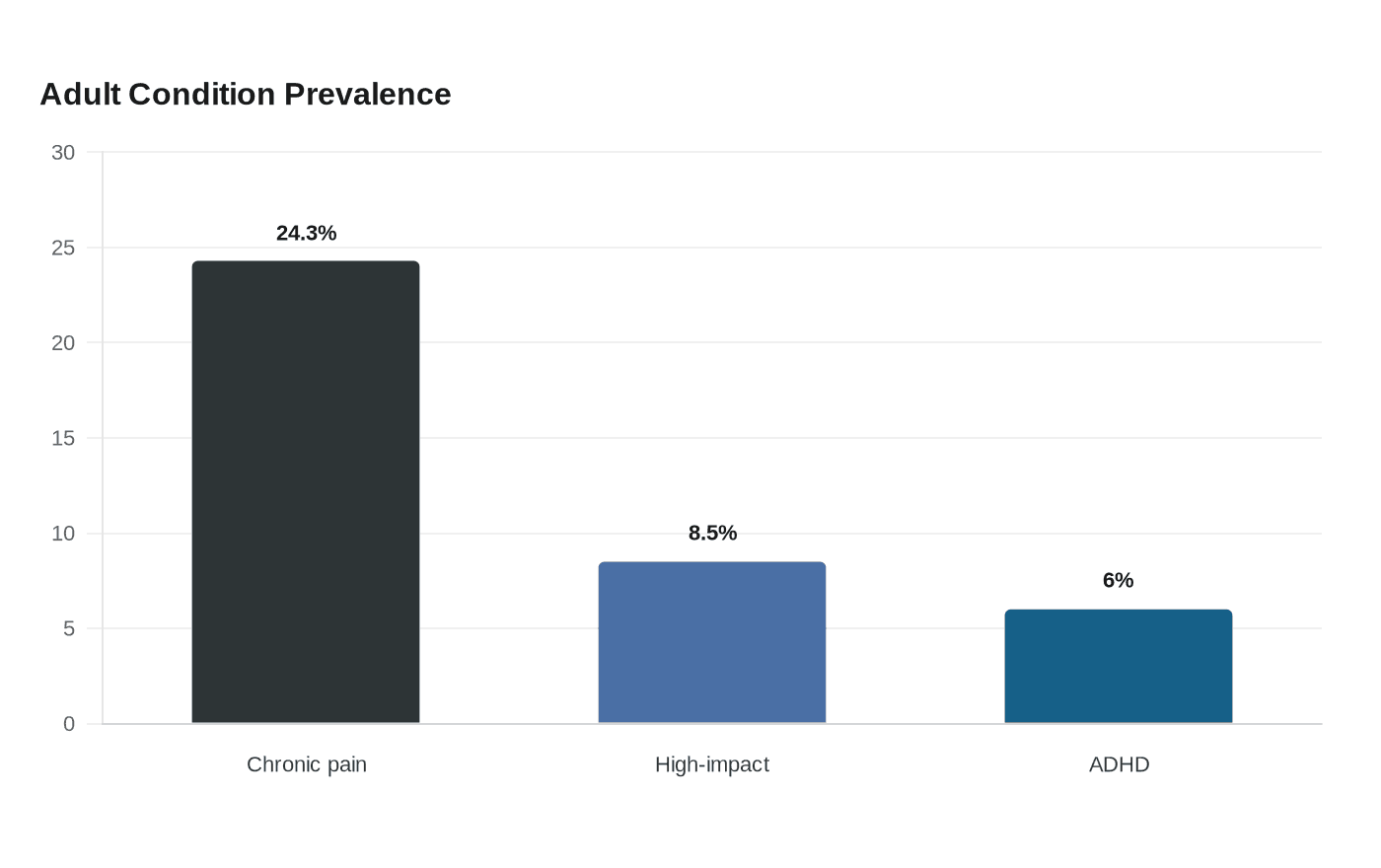
The scale of the problem is hard to ignore. The CDC reported that in 2023, 24.3% of U.S. adults had chronic pain and 8.5% had high-impact chronic pain, the kind that interferes with work and daily life. The agency defines chronic pain as pain lasting at least 3 months, and earlier CDC estimates found that about 50 million adults had it, with major health care and productivity costs.
ADHD is common too, and it often begins early. The National Institute of Mental Health says the median age of onset for children with current ADHD was 6 years, while CHADD cites an estimate that 15.5 million U.S. adults, or 6.0%, had a current diagnosis based on 2023 survey data. That means many people spend years navigating attention problems, impulsivity, or restlessness before chronic pain enters the picture, or vice versa, without anyone putting the two together.
Where the evidence is strongest
The newest research does not say ADHD causes chronic pain. What it does show is a consistent overlap that appears across several kinds of pain conditions, suggesting the connection is not just a coincidence in one specialty or one patient group.
A 2026 scoping review reported comorbidity not only in widespread pain syndromes such as fibromyalgia, but also in site-specific conditions including chronic low back pain, orofacial pain, and migraine. That matters because it broadens the clinical lens. ADHD is not just turning up alongside diffuse pain complaints, it is also showing up in conditions that have long been treated as separate problems with separate pathways.

A 2024 cross-sectional study found ADHD was more prevalent among psychiatric outpatients with chronic pain than among those without chronic pain. A 2025 genetic study then found significant genetic relationships between ADHD, migraine, and multisite chronic pain, strengthening the case that shared biology may be part of the story. Taken together, those findings suggest the overlap is visible in real-world patients and in the genome itself.
What researchers think may be happening
The leading explanations focus on brain systems that shape both attention and pain. Proposed mechanisms include dopaminergic and noradrenergic dysfunction, which may affect motor regulation, sensory processing, and descending pain modulation systems.
That framework makes clinical sense because pain is not only a signal from the body, it is also a brain-processed experience shaped by regulation, filtering, and response. If those systems are working differently in ADHD, then pain could be felt more intensely, managed less efficiently, or become more disruptive to daily function. The research is still developing, but the possibility of shared neurobiology is now strong enough that it should shape how clinicians think about both conditions.
Shared genetic factors may also help explain why ADHD and pain cluster together. The 2025 genetic findings do not prove direct causation, but they do suggest that inherited traits affecting brain development could raise the risk of both ADHD symptoms and pain vulnerability. That is an important distinction: the goal is not to turn every painful condition into an ADHD story, but to recognize that separate diagnoses may still share underlying pathways.
What remains uncertain
The biggest unanswered question is still whether ADHD directly causes chronic pain. The current evidence does not establish that link, and the association may reflect shared genetics, shared brain circuitry, or other overlapping vulnerabilities rather than a one-way cause-and-effect relationship.
Controlled trials are also scarce. Some case-based reports have described improved pain outcomes after ADHD-targeted pharmacotherapy, but those reports are not enough to guide broad treatment decisions on their own. Without larger controlled studies, it is too early to say whether treating ADHD reliably improves pain, which patients might benefit, or which pain conditions respond most strongly.
That uncertainty is not a reason to dismiss the overlap. It is a reason to stop treating the two conditions as if they live on separate clinical planets. When pain and attention symptoms travel together, the diagnostic workup should be broader, not narrower.
What clinicians should screen for
The practical lesson is simple: screen in both directions. Patients with chronic pain, especially fibromyalgia, chronic low back pain, migraine, or orofacial pain, may warrant questions about longstanding attention problems, disorganization, impulsivity, and childhood-onset symptoms. Patients with ADHD may also need routine questions about chronic pain, headache burden, jaw pain, back pain, and the degree to which pain is affecting work and daily activities.
That approach matters for care planning. Chronic pain is already a major public health burden, and ADHD can complicate treatment adherence, symptom tracking, and the ability to follow multi-step care plans. If clinicians see only one condition, they may miss part of the reason a patient is struggling.
It also matters for equity. Chronic pain is often dismissed, especially when it is invisible, fluctuating, or layered with psychiatric symptoms. People whose pain is not taken seriously can end up cycling through specialists without a cohesive plan, while ADHD symptoms can be mistaken for nonadherence, stress, or emotional distress rather than a treatable neurodevelopmental condition.
What patients should bring up
A more complete history can change the conversation. If pain has been present for years, if migraines or back pain coexist with lifelong distractibility, or if symptoms began in childhood and were never fully evaluated, those details deserve attention. The same is true if ADHD treatment has helped focus but pain remains unexplained, or if pain treatment has not improved function as expected.
Patients can also ask a direct question: could these symptoms be connected? That question is not a diagnosis, but it can open a better clinical workup. In a system that often separates neurology, psychiatry, and pain medicine, asking for a broader view can be the difference between fragmented care and a plan that fits the whole patient.
The emerging picture is not that ADHD is really a pain disorder, or that chronic pain is secretly ADHD. It is that the overlap is real, common enough to matter, and biologically plausible enough to take seriously. The next step is to build care around that reality, not the old habit of treating each diagnosis in isolation.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


