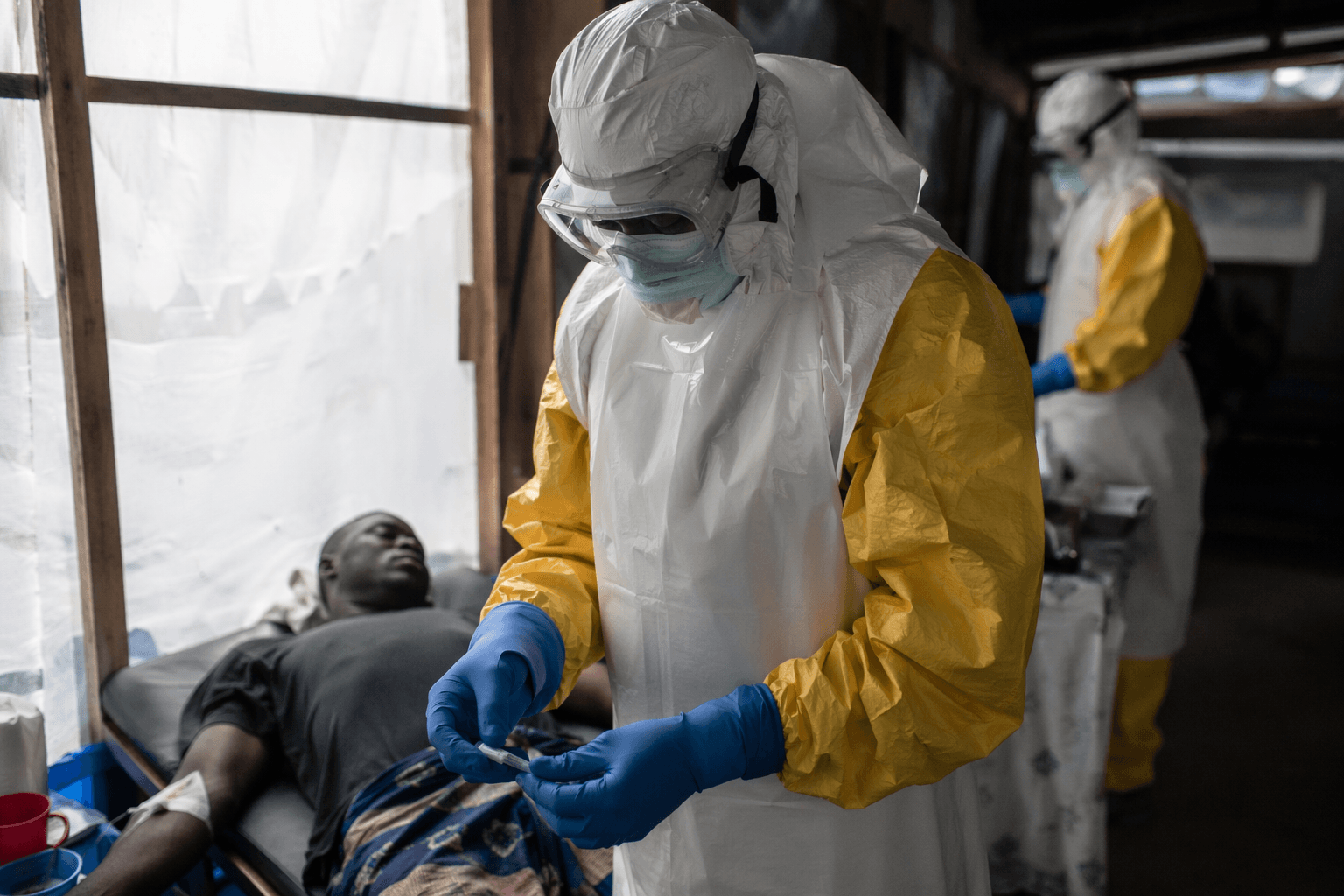
Ebola outbreak in Congo exposes deadly gap in rapid testing
Bunia’s first Ebola tests missed the Bundibugyo strain, leaving Congo with 500 suspected cases and only 30 confirmations as the outbreak spread.

A laboratory mismatch in Bunia helped turn Congo’s latest Ebola flare-up into a test of the global health system. Local tests initially came back negative for the more common Zaire strain, and only testing in Kinshasa identified the Bundibugyo virus, leaving doctors and responders chasing a pathogen they could not quickly name.
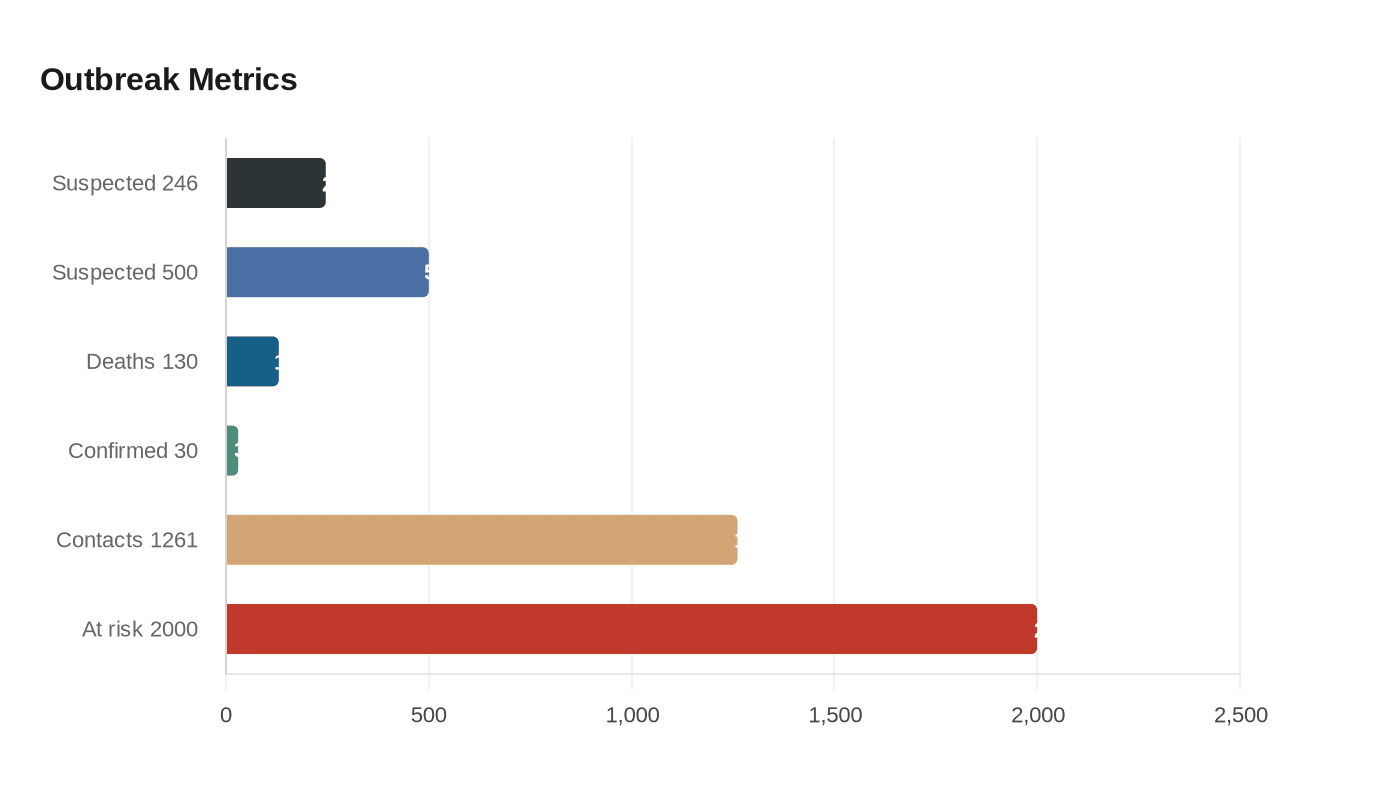
That delay mattered because the numbers were already climbing. On May 19, 2026, the World Health Organization said the Democratic Republic of the Congo had more than 500 suspected cases and 130 suspected deaths, but only 30 confirmed cases. With the Bundibugyo strain carrying no licensed vaccine and no targeted treatment, every missed day of diagnosis made isolation, contact tracing and burial safety harder to deliver.
The outbreak spread in a setting where the basics of containment were already strained. Hospitals were attacked and isolation tents were burned by angry mobs reclaiming bodies of loved ones, making it harder to separate the sick from the healthy and to track exposure chains. WHO said it was rushing more testing kits to eastern Congo, but the response was already lagging badly, with the outbreak moving “weeks if not months” ahead of the public health effort. In one coordination meeting, only 7% of 1,261 identified contacts had been found and followed up, even as the number of contacts at risk rose to more than 2,000.
The fragility was not only medical. The International Rescue Committee said suspected cases jumped from 246 to 500 in just 96 hours in May, as surveillance began catching up with transmission that may have been spreading for some time. The group said U.S. government funding that had supported frontline health and outbreak preparedness work in eastern Congo ended in March 2025, and its programming in Ituri was cut from five health areas to two. Many facilities in affected areas were also operating without basic protective supplies.
WHO said the outbreak was the 16th Ebola outbreak in Congo since the virus was identified in 1976, a grim marker of how little the world has changed after repeated emergencies. The agency said the country’s most recent prior outbreak had been in Beni, North Kivu Province, in 2022, and that the 2025 Kasai outbreak had affected Bulape and Mweka health zones, home to around 3.5 million people. Congo had 2,000 doses of the Ervebo vaccine in stock for Ebola Zaire, but that product does not protect against Bundibugyo, underscoring the same problem at the center of the crisis: when diagnostics and countermeasures do not match the strain on the ground, a virus outruns the system built to stop it.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


