Ebola outbreak in eastern Congo worsens as response strains grow
Frontline crews in eastern Congo still lack ambulances, staff and isolation materials as Ebola spreads through insecure mining corridors and contacts remain untraced.

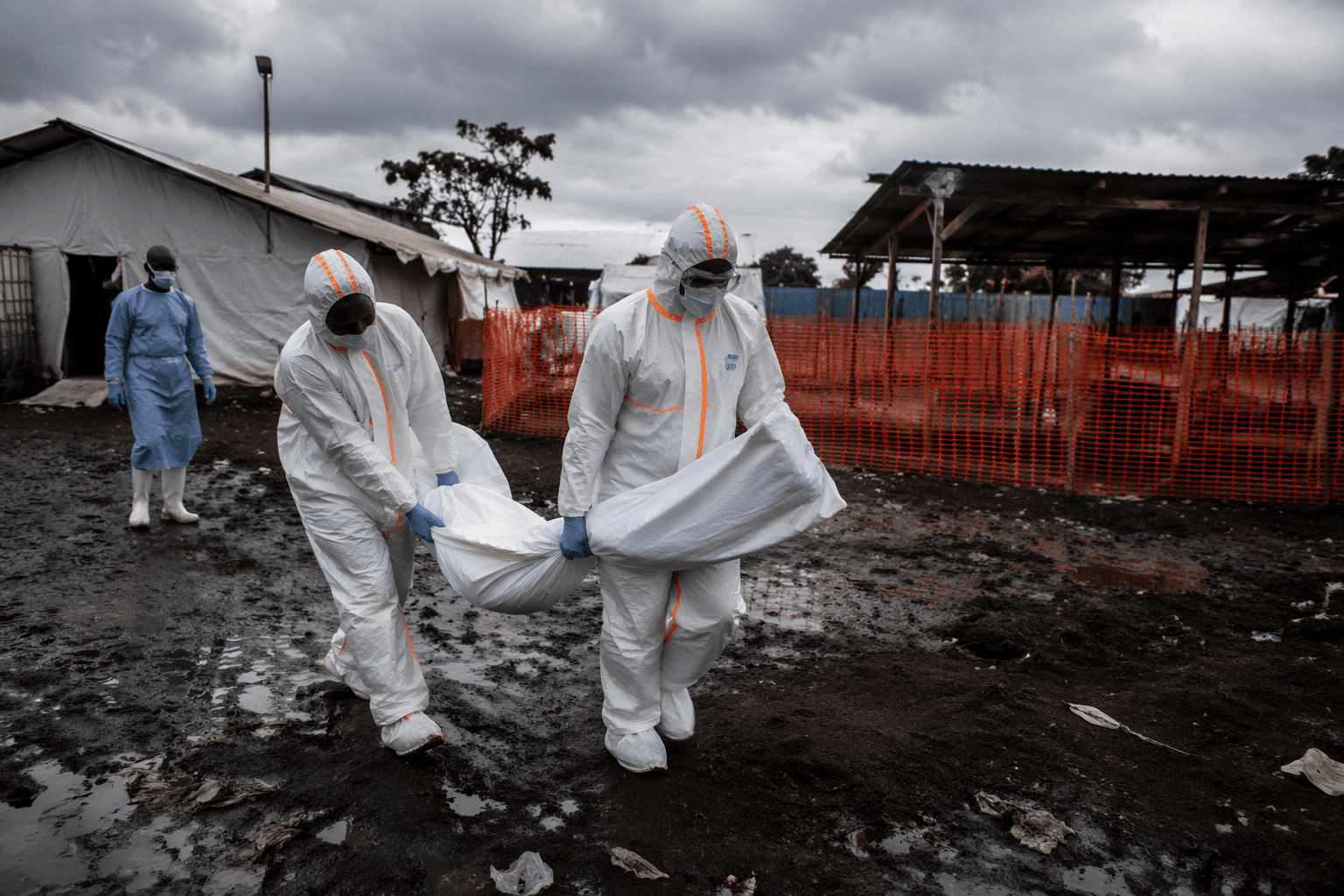
Frontline responders in eastern Democratic Republic of Congo are still short of personnel, ambulances and even basic construction materials for isolation wards, even as the Ebola outbreak spreads through an insecure, urban and mining-heavy corridor. One month after the World Health Organization escalated the crisis, the gap between global alarm and operational support is still defining the response.
The World Health Organization determined on 17 May 2026 that the Ebola disease caused by Bundibugyo virus in the Democratic Republic of the Congo and Uganda constituted a Public Health Emergency of International Concern, then convened its first emergency committee meeting two days later. WHO says the outbreak is unfolding in a humanitarian crisis context marked by insecurity, remote and densely populated areas, and heavy population and trade movements, while the Bundibugyo strain still has no vaccine or specific treatment. The response therefore depends on case finding, contact tracing, isolation, safe burials and fast logistics, all of them difficult to sustain in conflict-affected terrain.
Africa CDC moved just as quickly, declaring the outbreak a Public Health Emergency of Continental Security on 18 May 2026. Jean Kaseya, the agency’s director general, said tens of thousands of contacts remain untraced and warned that the outbreak is spreading where health teams cannot move safely. “After four weeks we have an outbreak in an urban area where there is insecurity,” he said. Africa CDC has highlighted high population mobility, insecurity, intense movement around Mongwalu, and gaps in contact listing and infection prevention and control.
Case counts have continued to climb. WHO said that by 27 May the Democratic Republic of the Congo had reported 906 suspected cases and 223 deaths among suspected cases. By 29 May, the agency said there were 134 confirmed cases across the DRC and Uganda, including nine in Uganda, with 18 deaths among confirmed cases. By 6 June, WHO said the DRC had 515 confirmed cases and 91 deaths among confirmed cases, while Uganda had 19 confirmed cases, two deaths and one probable death.
WHO has said Uganda’s outbreak is epidemiologically linked to transmission originating in the DRC, with evidence of imported infections and secondary transmission among contacts and healthcare workers. That cross-border spread has sharpened concern in Ituri province and beyond, including around Bunia, Rwampara and Mongwalu, where mining-linked mobility complicates surveillance and isolation.
On 8 June, the European Union announced an €11.5 million renewed commitment to support Africa CDC’s response. Africa CDC said on 9 June that experts were calling for stronger cross-border preparedness to reduce the risk of imported cases, while WHO continued to scale up support for surveillance, contact tracing, clinical preparedness, supplies, community engagement and border coordination. The outbreak now tests whether international warnings can be matched by the transport, staff and infrastructure needed to stop Ebola before it moves further.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Know something we missed? Have a correction or additional information?
Submit a Tip

