Inside Congo’s Ebola epicenter as the outbreak spreads across borders
A rare Ebola strain is moving through eastern Congo’s clinics and border towns, where insecurity and weak infrastructure are slowing containment.

Inside Ituri before the world is paying attention
The outbreak in eastern Congo is already showing the pattern that makes Ebola so hard to stop: a suspected cluster in a remote health zone, health workers among the earliest dead, and a virus moving faster than the system built to catch it. It was confirmed on May 15, 2026, in Ituri Province, centered in the Mongbwalu, Rwampara and Bunia health zones, and by then the country was confronting its 17th Ebola outbreak since 1976.
The first alarm came on May 5, when the World Health Organization was alerted to a high-mortality illness of unknown origin in Mongbwalu. The first known suspected case reportedly began symptoms on April 24, 2026, which means the virus had time to circulate before the response fully formed. By May 16, WHO said there were 8 laboratory-confirmed cases, 246 suspected cases and 80 suspected deaths in Ituri Province, a reminder that in the earliest days of an outbreak, the official tally can lag far behind what families and clinics are experiencing.
Why this outbreak is different from the usual Ebola playbook
This outbreak is caused by Bundibugyo virus disease, a rarer Ebola species. That matters because WHO says there is no licensed vaccine or specific treatment for this strain, leaving response teams to rely on isolation, infection prevention, surveillance and supportive care rather than a single medical fix. On May 17, the WHO Director-General declared the outbreak a Public Health Emergency of International Concern, signaling that the threat had moved beyond a local emergency.
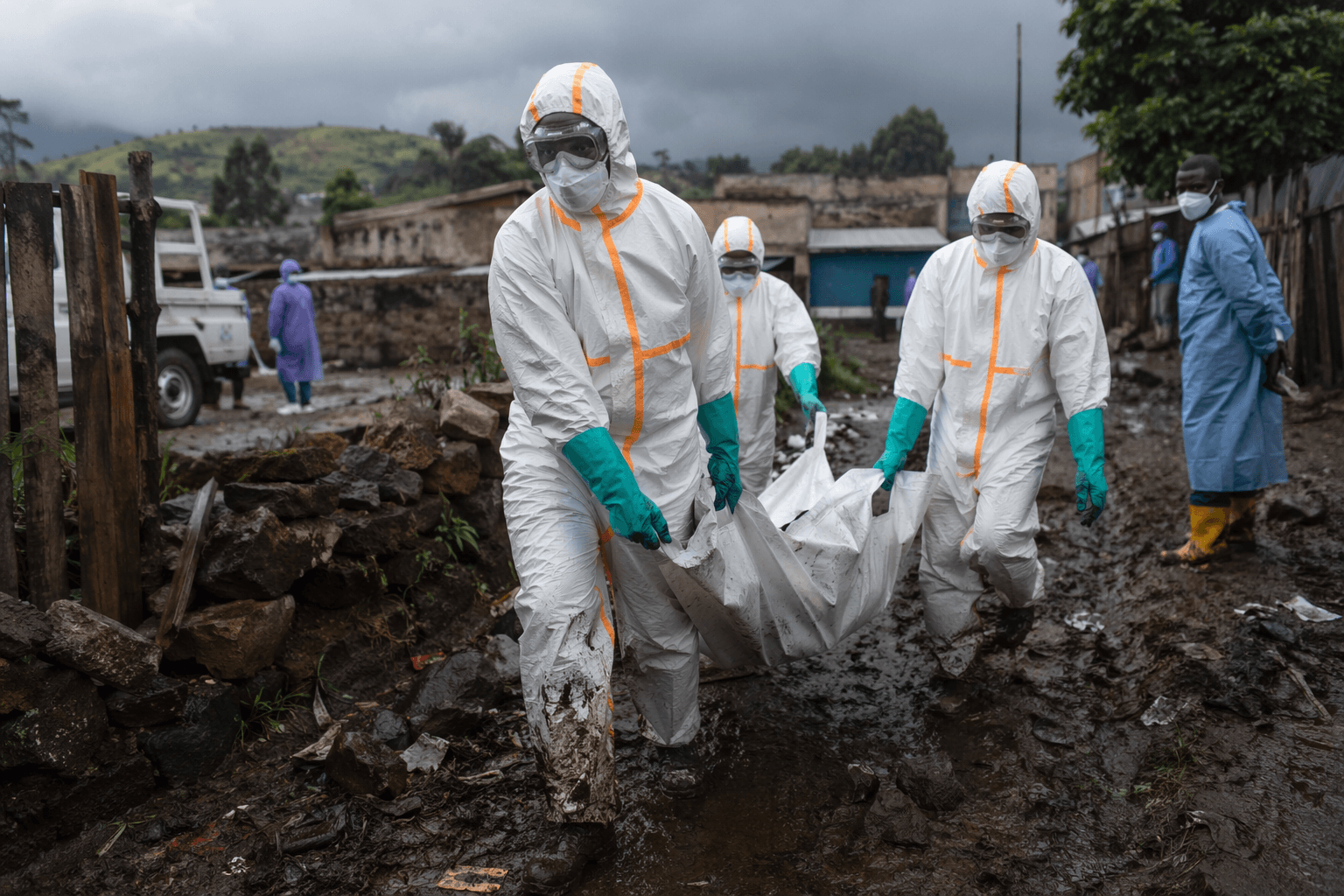
The challenge is not only biological. WHO says the situation is unfolding in a difficult setting marked by insecurity, high population mobility, cross-border and trade flows including mining, humanitarian strain and large refugee communities. Those conditions make the standard control tools, contact tracing, case isolation, safe transport of samples and rapid triage, far harder to execute. In places like Mongbwalu and Bunia, the gap between outbreak-control plans and daily reality is the real battlefield.
What the numbers say about the spread
The scale changed quickly. By May 29, WHO reported 134 confirmed cases across the Democratic Republic of the Congo and Uganda, including 9 in Uganda. Across both countries there had been 18 deaths among confirmed cases, while in the DRC alone there were 906 suspected cases and 223 suspected deaths. UNICEF said on May 18 that Uganda had already reported 2 cases and 1 death, which showed how quickly a local flare-up could become a cross-border concern.
That timeline matters because it shows the outbreak spreading through the same channels that keep eastern Congo economically connected: mining routes, trade corridors and constant movement across a porous border. The virus is not traveling through a vacuum. It is moving through communities where people already move because they must, for work, for safety and for survival.
How the response is being built on the ground
The response has depended on speed and logistics as much as medicine. WHO said it delivered 11.5 tonnes of medical supplies within 72 hours and deployed more than 35 experts and first responders, with airlift support from MONUSCO. UNICEF said it had mobilized nearly 50 tonnes of infection-prevention and control supplies to Bunia, where the response can stage equipment and supplies closer to the affected health zones.
Laboratory work has been central to narrowing the outbreak from a vague illness to a confirmed Ebola event. On May 14, the Institut national de recherche biomédicale analyzed 13 blood samples and confirmed Bundibugyo virus disease in eight. That is the point where response shifts from suspicion to containment, but it does not instantly solve the problems on the ground. In a province facing insecurity and stretched health services, diagnosis is only the first step in a much longer chain of care.
Why children and families face the deepest strain
UNICEF warned on May 18 that children are especially vulnerable because Ebola can disrupt essential services, separate families and increase psychosocial and protection risks. That warning is especially important in a place where schools, clinics and family networks are already under pressure from conflict and displacement. When a household loses trust in a clinic, or when travel to care becomes dangerous, the outbreak spreads through fear as well as contact.
UNICEF also said the virus may have started circulating in late April, which means some of the hardest choices came before communities had clear answers. Families faced illness without certainty, while health workers had to act before labs could confirm the disease. That lag is one of Ebola’s most dangerous features: by the time an outbreak is named, it has often already reshaped daily life.

What the cross-border response means now
Uganda’s involvement turns this from a provincial emergency into a regional test. The outbreak has already crossed into a second country, and the border does not respect the boundaries of ministry jurisdiction, aid planning or public anxiety. The Ministry of Public Health, Hygiene and Social Welfare in Congo, the Ministry of Health of Uganda and partners including WHO, UNICEF and MONUSCO now have to operate as if the virus will exploit every delay, every roadblock and every weak link in the chain.
For the wider world, the most immediate message is reassurance, not alarm. On June 1, 2026, the CDC said no Ebola cases from this outbreak had been confirmed in the United States and the risk to the American public and travelers remains low. But the deeper lesson is less comforting: outbreaks are usually won or lost far from global attention, in places where clinics are thinly staffed, roads are poor and trust can break faster than an ambulance can arrive.
The containment effort in Ituri is still in its hardest phase. The outbreak is already a regional crisis, and the next decisive factor will be whether those racing supplies, field teams and laboratory results can outpace the conditions that made Ebola possible there in the first place.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


