Modified CAR-T therapy may spare blood cancer patients toxic chemotherapy
A stem-cell memory CAR-T approach produced 45% complete responses without pre-treatment chemotherapy, hinting at a gentler path for hard-to-treat blood cancers.
A modified CAR-T therapy built from stem-cell memory T cells delivered complete remissions in a small first-in-human study without the harsh chemotherapy that normally prepares patients for treatment, a result that could make the cancer therapy easier to tolerate for some people with advanced blood cancers.
The study, published in Cell, tested a CAR-T product made from stem-cell memory T cells, or TSCM, a rare T-cell subset prized for self-renewal and long-term persistence. Patients in the trial had a range of blood cancers and had already failed bone marrow transplant treatment. No participant received chemotherapy before infusion, a striking departure from standard CAR-T practice.
Results were mixed but encouraging. Complete response rates were 45% in the TSCM group versus 10% in the standard CAR-T cohort, while overall response rates were statistically similar. One report said the standard cohort received a median dose of 290 million modified cells, compared with 66 million in the memory-stem-cell group. Another highlighted responses at doses as low as 250,000 cells per kilogram.

The modified cells also appeared to persist longer. Researchers reported a median time to adverse events or disease progression of 3.3 months in the standard CAR-T cohort and 4.9 months in the CAR-T stem-cell cohort. Four TSCM recipients went more than two years without disease progression. The memory-stem-cell group also showed lower rates of a common inflammatory reaction tied to overactive CAR-T cells, one of the best-known risks of the treatment.
Luca Gattinoni of the Leibniz Institute for Immunotherapy in Regensburg, Germany, led the study, with James Kochenderfer of the National Cancer Institute as co-corresponding author. Gattinoni said the findings open a new chapter in CAR-T design. Institutional coverage from the Leibniz institute said the results validate years of preclinical work, while stressing that the approach remains early.
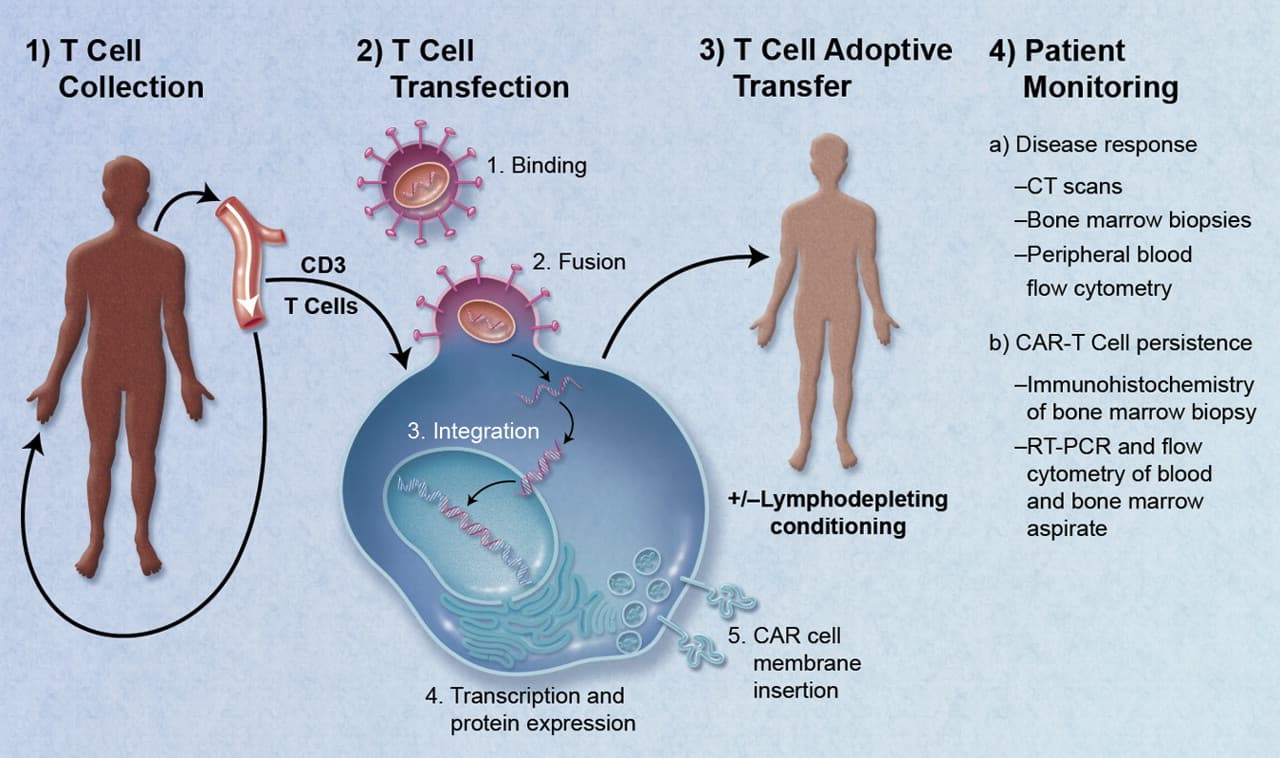
That caution matters. CAR-T has become part of modern cancer care over the past decade, but it still does not work for everyone. The Food and Drug Administration first approved a CAR-T therapy in 2017 for children with acute lymphoblastic leukemia, and later approvals expanded to adult blood cancers including non-Hodgkin lymphoma and multiple myeloma. The treatment uses a patient’s own T cells, engineers them to recognize cancer and returns them to the body as what the National Cancer Institute has called a “living drug.”
If larger studies confirm the early signal, the biggest payoff may be practical as much as scientific. Avoiding or reducing pre-treatment chemotherapy could lower complications, shorten preparation, and broaden access for frailer patients who have already been through extensive therapy. For now, the new data suggest a path toward a less punishing version of one of oncology’s most powerful tools.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


