Older transplant recipients with heart disease face higher Klebsiella risk
Heart disease and ICU stays of three days or more doubled Klebsiella risk in transplant recipients over 50, pointing to earlier surveillance in the first 180 days.

Older solid-organ transplant recipients with cardiovascular disease and longer ICU exposure faced a sharply higher risk of Klebsiella infection in the first 180 days after surgery, a signal that could help hospitals flag vulnerable patients before infection takes hold.
In a multicenter, retrospective case-control study at three hospitals in Greece and Italy, researchers examined transplant recipients older than 50 and found that a history of cardiovascular disease, along with a post-transplant ICU stay of at least three days, was each associated with more than a twofold increase in Klebsiella risk. The study looked at infection episodes within 180 days of transplantation, a period when anti-rejection drugs and post-operative complications can leave patients especially exposed.

The practical value of the finding is in the pattern it reveals. Cardiovascular disease may mark greater medical complexity, frailty, or a harder post-operative course, while a prolonged ICU stay can reflect both severe illness and more contact with invasive devices and hospital flora. Together, those factors could help transplant teams identify older recipients who need tighter infection surveillance, earlier microbiology testing if fever or graft dysfunction appears, and more careful line management.
That matters because Klebsiella spp. are a major cause of antimicrobial-resistant hospital-acquired infections. In transplant medicine, where immune suppression is deliberate and unavoidable, even routine post-operative exposure can become dangerous. The early months after surgery are already one of the most fragile stretches in the entire care pathway, and the new data suggest that baseline heart disease and critical-care duration should be treated as warning signs, not background information.

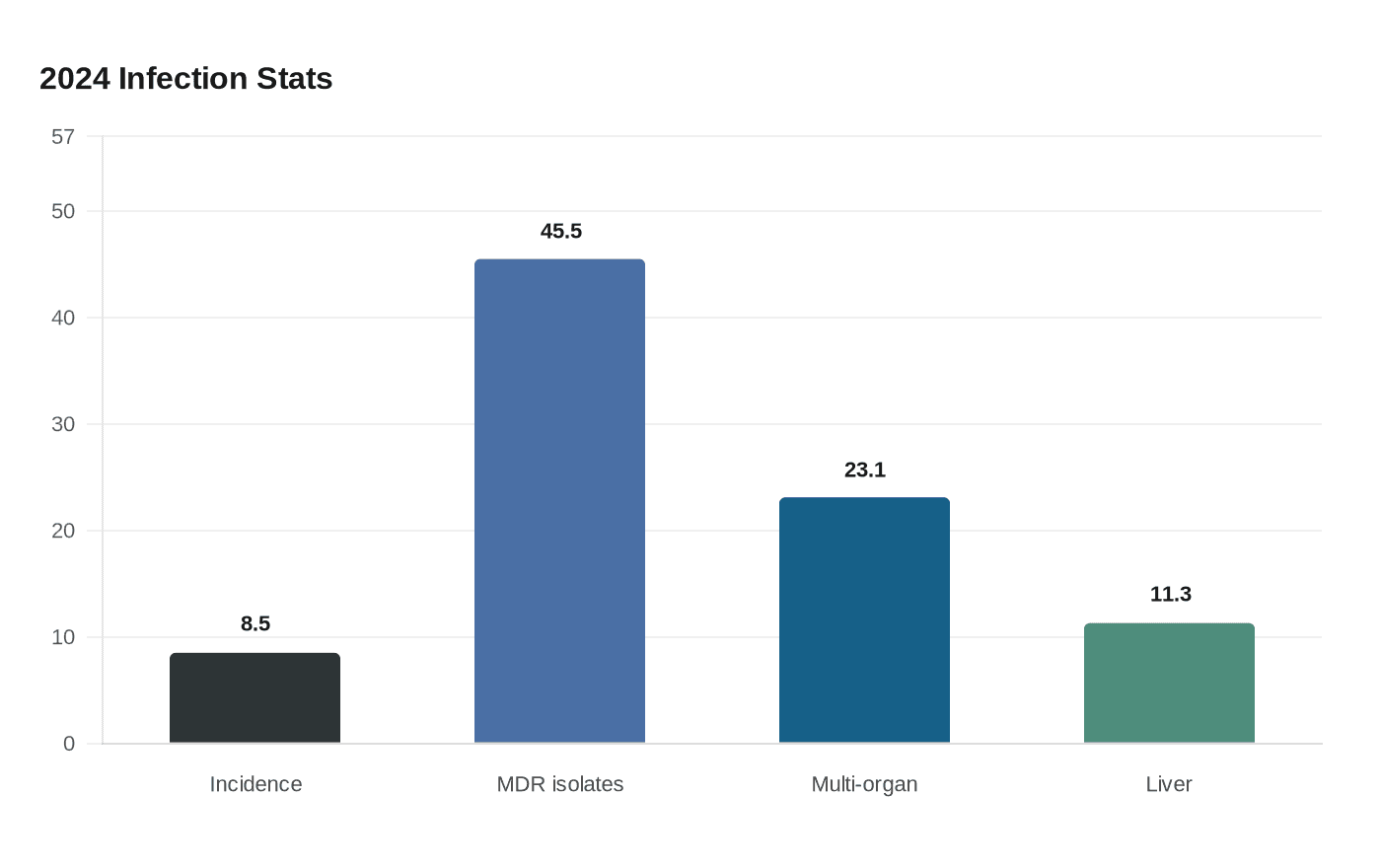
The broader literature points in the same direction. A 2024 study of bloodstream infections after solid-organ transplantation found an 8.5% incidence in the first year after transplant, and 45.5% of unique isolates were multidrug-resistant. Bloodstream infections were most common after multi-organ transplantation, at 23.1%, and after liver transplantation, at 11.3%.
Even when donor-derived transmission is involved, the risk is rare. CDC guidance says infection transmission through transplantation occurs in less than 1% of all transplants, but rapid notification and treatment can improve survival and help preserve the graft when it is suspected. Prior reports have documented donor-derived multidrug-resistant Klebsiella pneumoniae bacteremia in liver and kidney recipients, and a 2022 to 2023 study found carbapenem-resistant Klebsiella pneumoniae in solid-organ transplant recipients carried significant morbidity and mortality.
For transplant centers, the lesson is straightforward: prevention does not end in the operating room. In older recipients, especially those with cardiovascular disease and a prolonged ICU stay, the safest course may be earlier surveillance, faster testing, and tighter infection-control discipline during the months when recovery remains most fragile.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


