Study finds early GLP-1 use in pregnancy not linked to major risks
Accidental first-trimester GLP-1 exposure did not show major risk signals in 3,572 pregnancies, but experts still advise stopping the drugs once pregnancy is known.
A new Harvard-led analysis is offering some reassurance to patients who discover they were taking a GLP-1 drug before realizing they were pregnant. In 3,572 pregnancies drawn from U.S. insurance claims, continuing the medication into the first trimester was not linked to a statistically significant rise in non-live birth, low birth weight, high birth weight or major congenital malformations.
The study, published in Annals of Internal Medicine and based on Merative MarketScan data from 2011 to 2024, looked at pregnant women ages 16 to 55 who had filled a GLP-1 receptor agonist prescription in the 90 days before their last menstrual period. Of the pregnancies studied, 1,467, or 41.1 percent, were among women with type 2 diabetes, a group in which medication decisions can be especially complex because pregnancy itself raises the stakes for glucose control.
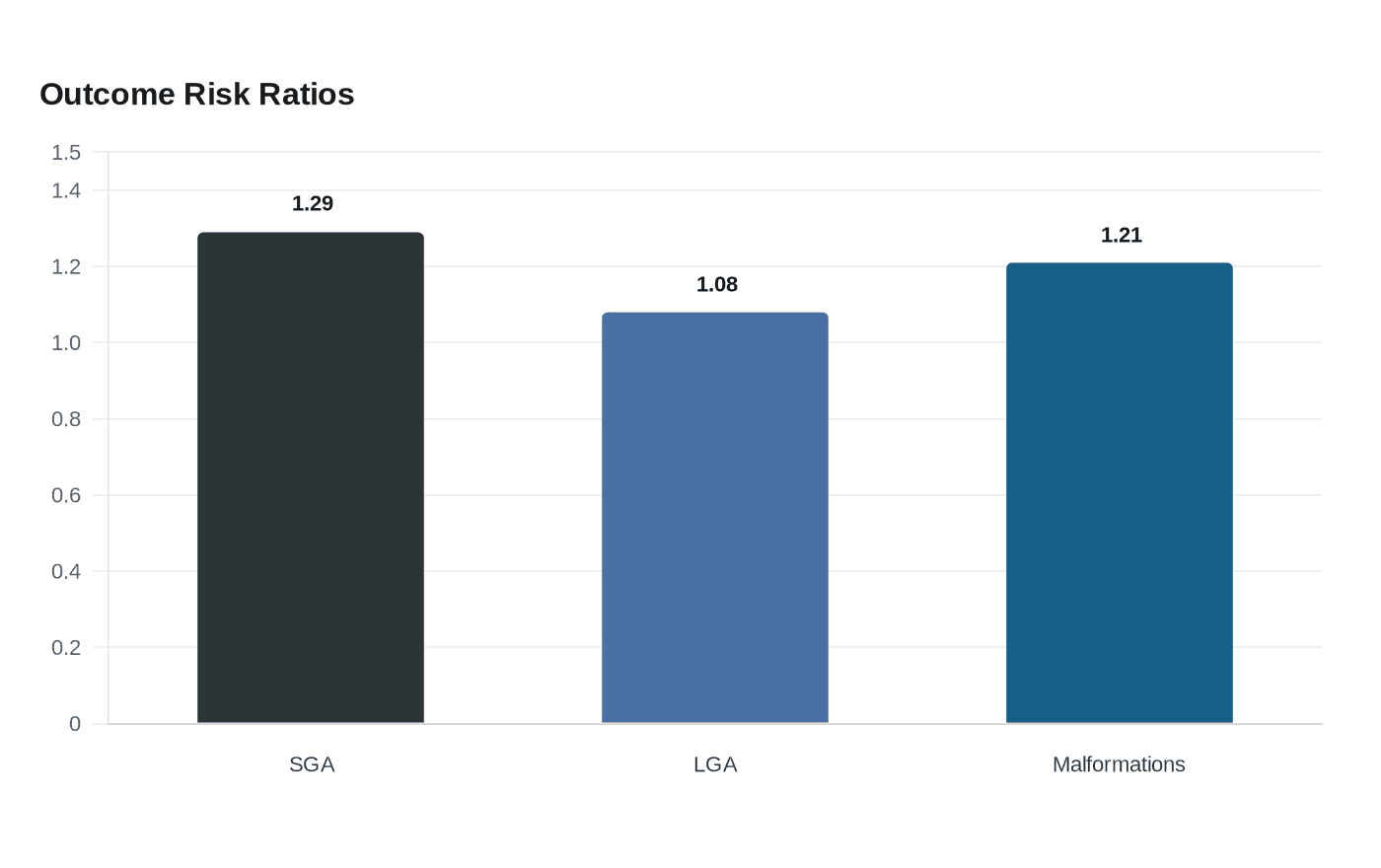
Researchers compared women who kept taking the drugs in early pregnancy with those who stopped. The rate of non-live birth was 29.7 percent in the continuation group and 27.1 percent in the noncontinuation group, a difference that was not statistically significant. Among 2,529 live-birth pregnancies, 1,499 infants were linked for analysis. The weighted prevalence ratios were 1.29 for small for gestational age, 1.08 for large for gestational age and 1.21 for major congenital malformations, with confidence intervals crossing 1.0.
That is reassuring, but not a green light to stay on these medications during pregnancy. The authors said the study could still be affected by residual confounding from prior glycemic control, and fetal safety remains uncertain. Animal studies have raised concerns, and the U.S. Food and Drug Administration label for Zepbound says to discontinue it when pregnancy is recognized and warns that it may cause fetal harm.
The warning matters because GLP-1 use has surged among women of reproductive age, increasing the chances of surprise exposures. The Zepbound label also tells women using oral contraceptives to switch to a non-oral method or add a barrier method for four weeks after starting tirzepatide and for four weeks after each dose increase, a safeguard that helps explain how unplanned pregnancies can happen while people are on treatment.
The new findings build on earlier Harvard research published in December 2023, which found no greater risk of major congenital malformations when women with pregestational type 2 diabetes used second-line non-insulin antidiabetic drugs, including GLP-1 receptor agonists, rather than insulin across more than 3.5 million pregnancies in Finland, Iceland, Norway, Sweden, the United States and Israel. A separate JAMA cohort study published online in November 2025 found that people who stopped GLP-1 drugs before or in early pregnancy had 3.3 kilograms greater gestational weight gain than unexposed pregnancies, underscoring the maternal tradeoffs clinicians must weigh. The message now is careful and clear: accidental early exposure does not appear to demand panic, but planned discontinuation and preconception counseling still matter.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Know something we missed? Have a correction or additional information?
Submit a Tip

