HerStack names best perimenopause care pathways for 2026
HerStack’s 2026 pathway starts with symptom-led diagnosis, not routine hormone tests, then routes women to HRT, vaginal estrogen or non-hormonal options by symptom cluster.
For most women in their 40s with hot flushes, night sweats and cycle changes, the best pathway is symptom-led diagnosis first, then treatment matched to the symptom cluster, because routine hormone testing is usually not the starting point. HerStack grades that as the sensible default, and its care page routes readers through the NHS, private menopause clinics and UK telehealth instead of pretending one route fits everyone.
The symptom list is wider than the headline version people usually hear. NHS and NICE materials, along with Alberta Health Services and PMC reviews, describe perimenopause as a mix of menstrual changes, hot flushes, night sweats, mood shifts, sleep disturbance, cognitive complaints, joint pain and genitourinary symptoms such as vaginal dryness, urinary frequency and pain with sex. The NHS says menopause and perimenopause usually affect women between 45 and 55, while NICE says people aged 45 or over with typical symptoms can usually be diagnosed from clinical history alone.
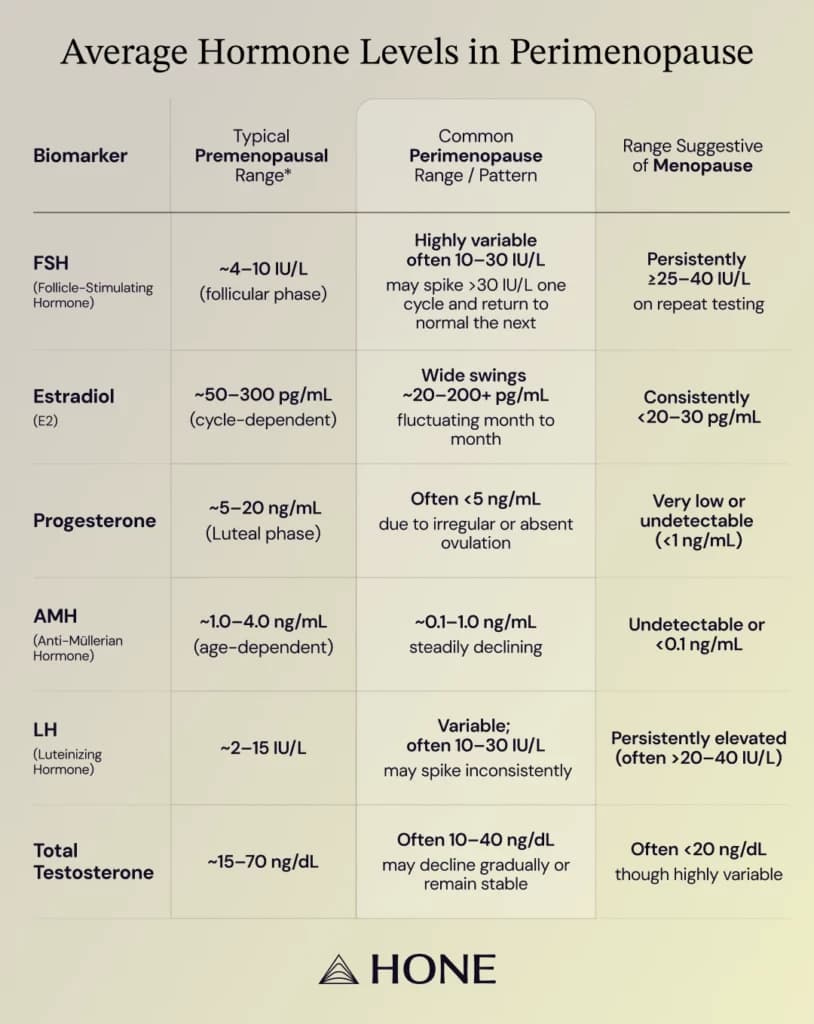
That is why the strongest evidence-backed route still starts with the story the body is telling, not a broad hormone panel. Mayo Clinic says there is no single test for perimenopause and that hormone testing is usually not helpful, other than checking for thyroid disease when the history suggests it; NICE’s 2026 update keeps diagnosis centred on age, symptoms and menstrual pattern. If the dominant problem is vasomotor symptoms, systemic estrogen remains the most effective treatment, usually with progestogen if the uterus is present; if the problem is vaginal dryness or urinary symptoms, local vaginal estrogen is the targeted option. Non-hormonal choices such as SSRIs, gabapentin, oxybutynin and fezolinetant remain the main alternatives when estrogen is not suitable or not wanted.
HerStack’s value is that it behaves like an editorial filter, not a clinic brochure. Its own site says it is an independent editorial resource, its concern-finder takes seven questions in about 90 seconds, and its care pathway explains how NHS care, private menopause clinics and UK telehealth differ before you book anything. That is a different job from Newson Health, which says it was founded by Dr Louise Newson and Dr Rebecca Lewis in 2018 and offers in-person and virtual consultations, or My Menopause Centre, which says appointments are available within days at £290 for doctor-led visits or £190 for nurse-led visits. The Better Menopause is a supplement brand, not a care pathway, and sells science-backed products for sleep, digestion and metabolic symptoms.
The places where the pathway should get sharper are also the places where good clinicians already get cautious. NICE and the NHS both treat unscheduled or postmenopausal bleeding as a reason to seek medical review, and the NHS says postmenopausal bleeding should be checked by a GP, with specialist assessment often within two weeks. NICE updated its advice on vaginal bleeding while taking systemic HRT in April 2026, which is the kind of detail that matters when a midlife patient is deciding whether a symptom is an expected side-effect or a red flag. Complex symptoms, bleeding that persists, or perimenopause before 40 still deserve a clinician, because the best pathway is the one that keeps diagnosis precise and avoids unnecessary testing. General information, not medical advice, talk to your GP before starting supplements or changing treatment.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


