Randomized Trial Finds Yoga with Buprenorphine Shortens Withdrawal Time, Improves Symptoms
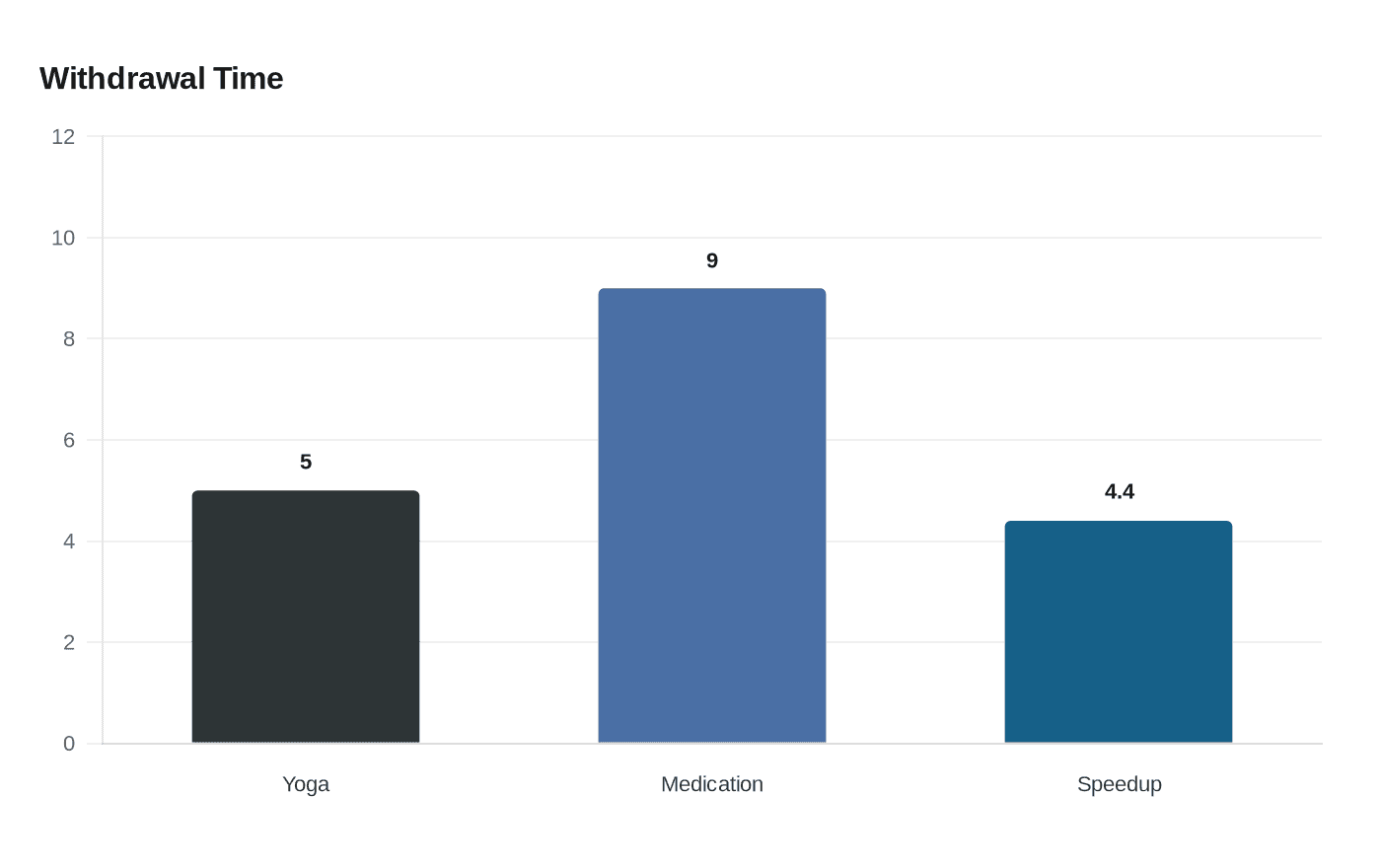
A randomized trial found that adding a brief supervised yoga program to buprenorphine shortened withdrawal stabilization from about nine to five days and improved HRV, anxiety, sleep, and pain.

A randomized clinical trial led by investigators at the National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, with collaborators from Harvard Medical School found that a targeted yoga program added to standard buprenorphine treatment substantially shortened time to opioid withdrawal stabilization and improved physiological and symptom measures.
Fifty-nine men with opioid dependence were randomized to receive buprenorphine alone or buprenorphine plus a short, supervised yoga intervention. The yoga package delivered 10 supervised sessions over roughly two weeks and combined breathwork (pranayama), gentle postures, and brief guided relaxation and meditation including Yoga Nidra elements. The primary outcome was median time to withdrawal stabilization, and the yoga-plus-medication group reached stabilization in about five days versus about nine days in the medication-only group. The study reported an effect estimate indicating the yoga group achieved stabilization roughly 4.4 times faster.
Researchers also measured heart rate variability as an index of autonomic balance and found improvements in HRV among participants who practised yoga, suggesting improved parasympathetic regulation. On patient-reported measures, participants assigned to yoga reported reductions in anxiety, faster sleep onset and overall sleep improvement, and lower pain scores compared with controls. The trial authors listed on the report include Goutham S., Bhargav H., Holla B., et al., with the findings published in JAMA Psychiatry.
For yoga teachers, clinicians, and community programs, the results give concrete, clinically measured evidence that breath regulation, mindful movement, and relaxation techniques can influence autonomic physiology and tangible clinical outcomes during the acute withdrawal phase. The intervention was short, low-cost, and structured, making it feasible to adapt into medication-assisted treatment settings or recovery programs that already coordinate clinical care. Trauma-informed and medically informed adaptations would be appropriate when working with people in withdrawal or early recovery.
The study carries important caveats. It was single-centre, included only male participants, had a relatively small sample size, and followed participants for a short period. Those limitations mean larger, multi-site trials with women and more diverse populations and longer follow-up are needed to confirm durability of benefits and any effects on relapse risk.
This trial frames yoga not only as a wellness practice but as a measurable adjunct in addiction care. For community programs, the next steps are practical: consider training modules in pranayama, gentle asana, and guided relaxation suitable for clinical settings, and seek collaborations with addiction treatment services to test scalable, trauma-informed models that preserve safety and clinical oversight.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


