Ebola outbreak tests U.S. preparedness as cases spread in Congo, Uganda
A fast-moving Bundibugyo Ebola outbreak in Congo and Uganda is testing whether U.S. surveillance, hospitals, and messaging can do more than improvise.

Why this outbreak is a stress test, not just a distant health crisis
The current Ebola outbreak in the Democratic Republic of the Congo and Uganda is forcing the U.S. public-health system to prove how much stronger it has become since COVID-19. The risk to the American public remains low, but federal agencies are already using enhanced travel screening, entry restrictions, and other measures to keep the virus from reaching U.S. soil. At the same time, the response is exposing a harder question: whether the country has built enough durable coordination, laboratory capacity, and hospital readiness to handle a truly dangerous importation without scrambling.
The outbreak is centered on Bundibugyo virus, a strain that does not currently have a licensed vaccine or specific treatment. That makes fast detection and isolation even more important, especially as the World Health Organization declared the outbreak a Public Health Emergency of International Concern on May 17, 2026, citing rising cases, cross-border spread, and uncertainty about the true scale of transmission.
What the numbers show
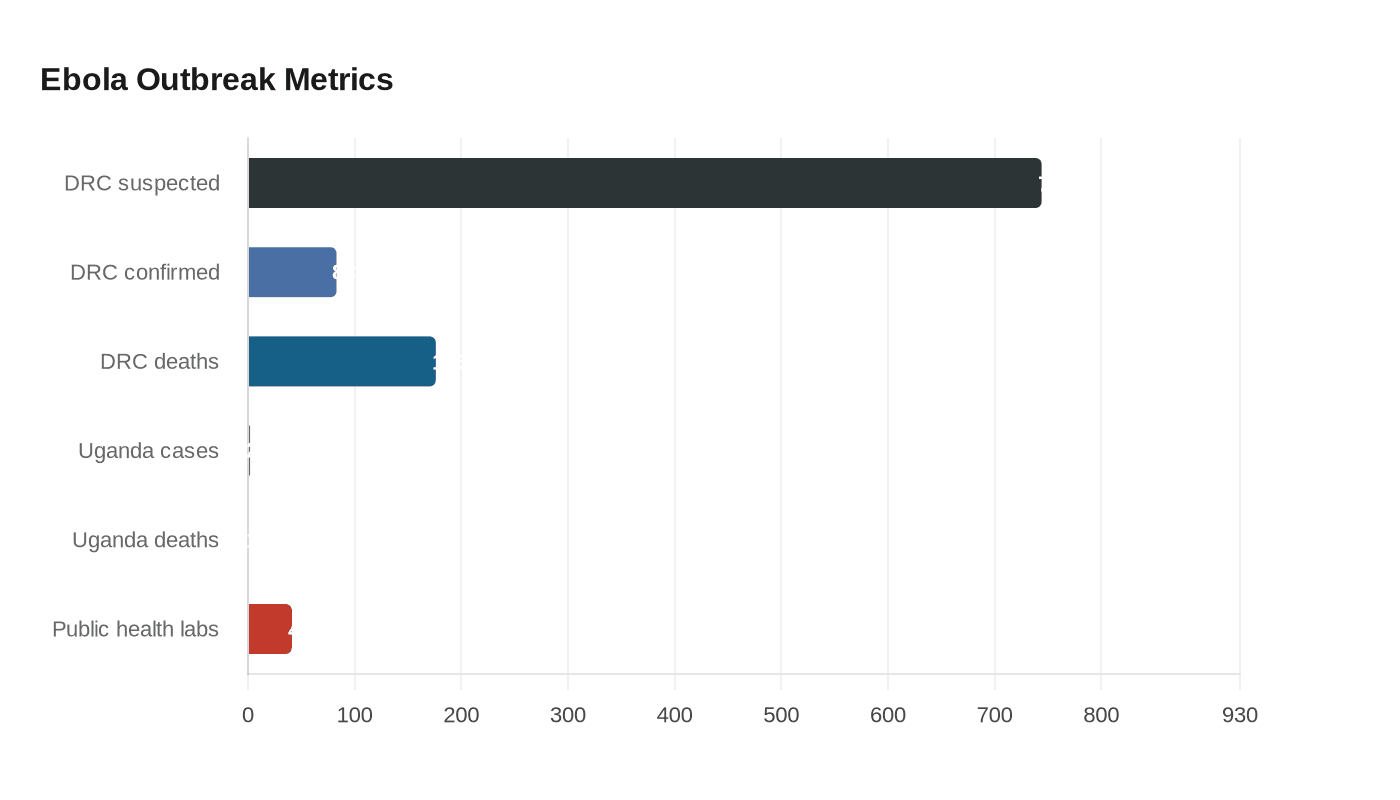
By May 22, the Centers for Disease Control and Prevention said the outbreak had reached 744 suspected cases, 83 confirmed cases, and 176 suspected deaths. CDC also reported a new confirmed case in Sud-Kivu Province, expanding the outbreak beyond the earlier focus in Ituri and Nord-Kivu provinces. Uganda has also seen spillover from travelers who had been in the DRC, with 2 confirmed cases and 1 death reported there.
Those figures matter because Ebola is not spreading evenly or predictably. The current pattern crosses borders, moves through hard-to-reach terrain, and is unfolding in a region where transport is limited and security conditions remain difficult. CDC says the DRC’s current outbreak is its 17th Ebola outbreak since 1976, and its second Bundibugyo outbreak, a reminder that this is not a one-off emergency but part of a recurring containment challenge.
How the U.S. response has changed
The federal response now looks far more structured than the improvisation that marked earlier crises. CDC says the agency has long-standing laboratory preparedness through the Laboratory Response Network, with 41 public health laboratories able to support testing. It is also coordinating with the Department of Homeland Security and other federal partners to prevent introduction of the virus into the United States.
That coordination became more visible on May 18, when CDC and DHS announced enhanced travel screening, entry restrictions, and additional public-health steps. The U.S. State Department then said on May 19 that it would fund up to 50 Ebola response clinics in affected areas of the DRC and Uganda, arguing that rapid containment and treatment capacity are critical in the first days of an outbreak. The message is clear: stop spread early, treat aggressively, and keep local health systems from being overwhelmed.
The United States also faced a direct exposure event of its own. On May 17, CDC said an American who had been caring for patients in the DRC tested positive for Ebola Bundibugyo disease and was evacuated to Germany for treatment. High-risk contacts were moved to Germany and the Czech Republic. That decision reflects the current playbook: isolate cases quickly, protect contacts, and avoid unnecessary exposure during transport or treatment.
Where preparedness still depends on improvisation
Even with better federal coordination, the system still depends on fast decisions and uneven local capacity. CDC’s laboratory network can identify the virus, but that only helps if hospitals recognize the risk early enough, collect specimens correctly, and follow infection-control protocols without delay. The outbreak is also a reminder that preparedness is not just about U.S. airports and federal labs. It depends on whether emergency rooms, infection-prevention teams, and public-health departments can move in lockstep when the first suspicious patient appears.
That is where the lessons from COVID still loom large. Screening at the border can reduce risk, but it cannot replace contact tracing, bed isolation, protective equipment, and clear clinical guidance once a case is suspected. The federal response has improved, yet it still leans on a chain of local judgment calls that can break under pressure if hospitals are understaffed or communication is inconsistent.
Why this strain is so concerning
Bundibugyo virus was discovered in 2007, and CDC says it causes death in about 30% of infections. That is lower than the Ebola virus that drove the 2014 to 2016 West Africa outbreak, which CDC describes as the largest on record, with more than 28,600 cases and a fatality rate that can reach up to 90% without treatment. The lower fatality rate should not lull policymakers into complacency. Bundibugyo still spreads through direct contact, still requires aggressive isolation, and still becomes more dangerous when health systems are delayed or disorganized.
WHO and U.N. News have stressed the basics that save lives in outbreaks like this: surveillance, contact tracing, laboratory testing, infection prevention, and engagement with local and religious leaders. They have also warned that at least four healthcare-worker deaths have raised concern about infection prevention and control. That is a red flag for any response, because when clinicians become casualties, the system starts losing the very people needed to contain transmission.
The politics of messaging and the memory of 2014
This outbreak is also a test of political messaging. The Washington Post reported that the administration’s reluctance to bring an infected American back to U.S. soil marked a sharp contrast with the 2014 West Africa Ebola outbreak, when the politics of repatriation and treatment were more visibly contested. That difference matters because public confidence depends on whether officials sound disciplined, transparent, and consistent when the threat is still small.
Former CDC Director Robert Redfield has warned publicly that the outbreak could become “a very significant pandemic,” capturing the anxiety among some public-health veterans that the world may be underestimating the situation. WHO, for its part, says the outbreak does not meet pandemic criteria under the International Health Regulations. Both points can be true at once: the outbreak may not qualify as a pandemic emergency, yet still demand urgent containment because cross-border spread and incomplete case counts make the true scale uncertain.
What to watch next
The next phase will hinge on four measures: whether case finding improves in the DRC and Uganda, whether hospitals and clinics can safely isolate and triage patients, whether contact tracing keeps pace with travel-linked spread, and whether U.S. screening and laboratory systems stay ahead of any imported case. The U.S. is better prepared than it was in the early days of earlier outbreaks, but the system still relies on rapid coordination, clear public communication, and local execution under pressure.
That is the real lesson of this Ebola outbreak. Preparedness is no longer just a promise made after a crisis. It is being measured now, in the speed of detection, the discipline of response, and the ability of public institutions to act before a distant outbreak becomes a domestic one.
Know something we missed? Have a correction or additional information?
Submit a Tip

