Gene-editing drug sharply lowers LDL in early heart study
A single CTX310 infusion cut LDL and triglycerides within two weeks in 15 patients, but the Phase 1 signal stops short of showing heart protection.
A one-time gene-editing infusion pushed LDL cholesterol sharply lower in a small first-in-human heart study, an early result that points to what investigators described as a possible long-duration treatment but still falls far short of proving disease prevention.
The experimental drug, CTX310, uses CRISPR-Cas9 to target angiopoietin-like protein 3, or ANGPTL3, in the liver. In the 15-patient Phase 1 trial, LDL cholesterol and triglycerides fell within two weeks of treatment and stayed low for at least 60 days, with follow-up still ongoing. Researchers reported that the therapy was well tolerated in short-term monitoring and that no serious adverse events were linked to the treatment during that early period.
The data were presented at the American Heart Association Scientific Sessions 2025 in New Orleans and published at the same time in The New England Journal of Medicine. Luke Laffin, a Cleveland Clinic cardiologist and the study’s first author, said the result was still very early in development but could eventually offer a safe, durable one-time infusion instead of a daily pill or frequent injection. Steven Nissen, Cleveland Clinic’s chief academic officer for cardiovascular medicine and the senior author, framed the work against a broader adherence problem, saying about half of patients prescribed cholesterol-lowering medicines stop taking them within a year.
The trial’s logic comes from human genetics. People born with naturally inactivated ANGPTL3 appear to have lower lifetime heart-disease risk without obvious harmful effects, which helped inspire the therapy. That same strategy has already shaped earlier gene-editing work in PCSK9, another pathway tied to LDL control. A 2024 review in European Heart Journal - Cardiovascular Pharmacotherapy described VERVE-101 data showing LDL reductions of up to 55% that persisted for six months in one dose cohort.
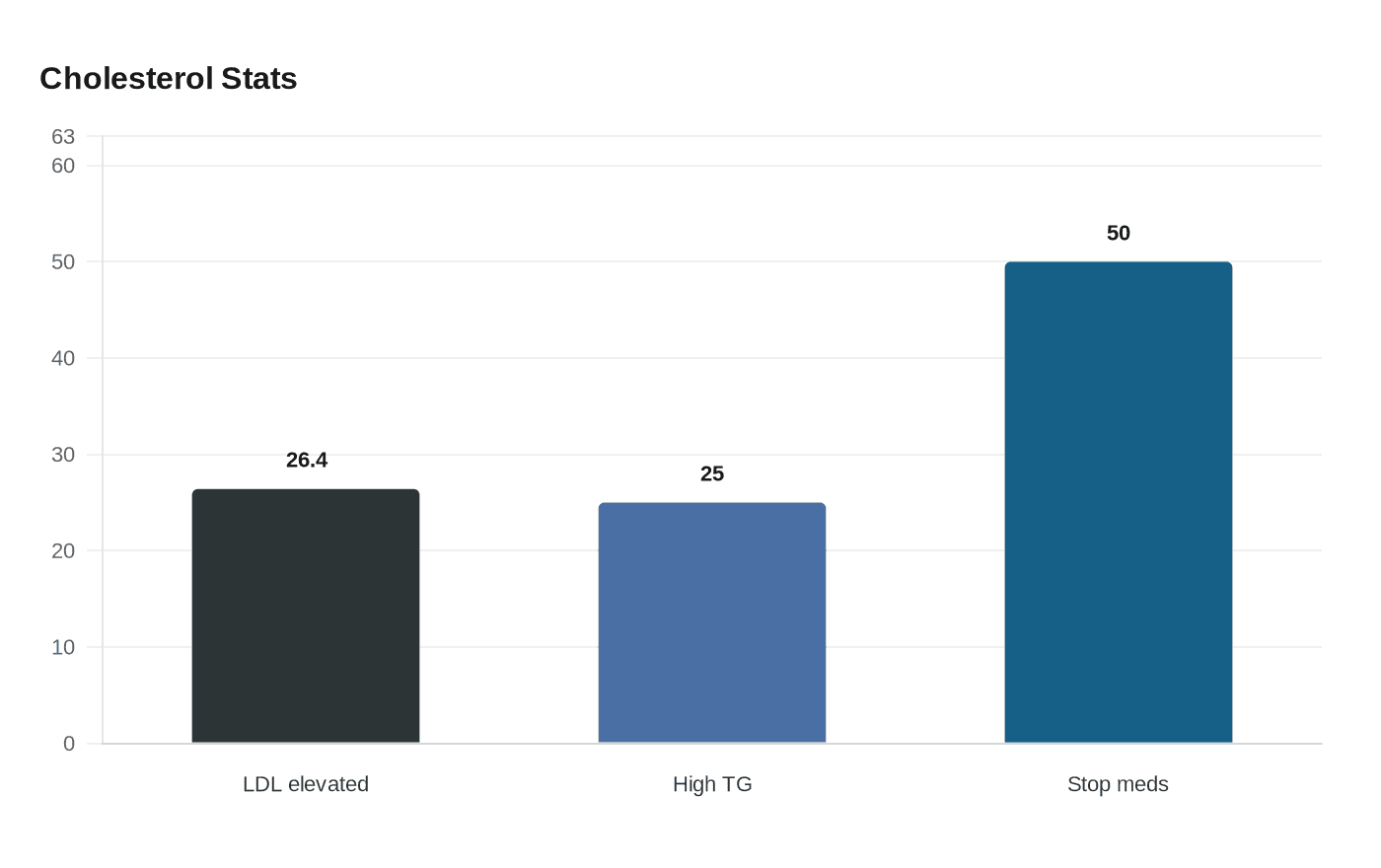
The promise is clear: if later studies confirm durability and safety, a one-time gene edit could be aimed at patients who cannot get LDL and triglycerides under control with standard therapy. Cleveland Clinic said that as of 2018, 26.4% of U.S. adults had elevated LDL cholesterol, and about 25% had high triglycerides, underscoring how large the treatment pool could be.
The limits are just as important. A Phase 1 study can show whether a treatment reaches its target and appears tolerable in a small group; it cannot show whether it prevents heart attacks or strokes, how long the effect lasts beyond the early follow-up window, or whether the approach can be delivered safely and affordably to broad populations. Larger and longer trials will have to answer those questions before a gene-editing heart drug can move from dramatic early signal to routine care.
Know something we missed? Have a correction or additional information?
Submit a Tip