Shingles vaccine may lower dementia risk in older adults
A newer shingles shot is increasingly linked to lower dementia risk, but the evidence is still observational. The findings strengthen prevention hopes without changing vaccine guidance yet.
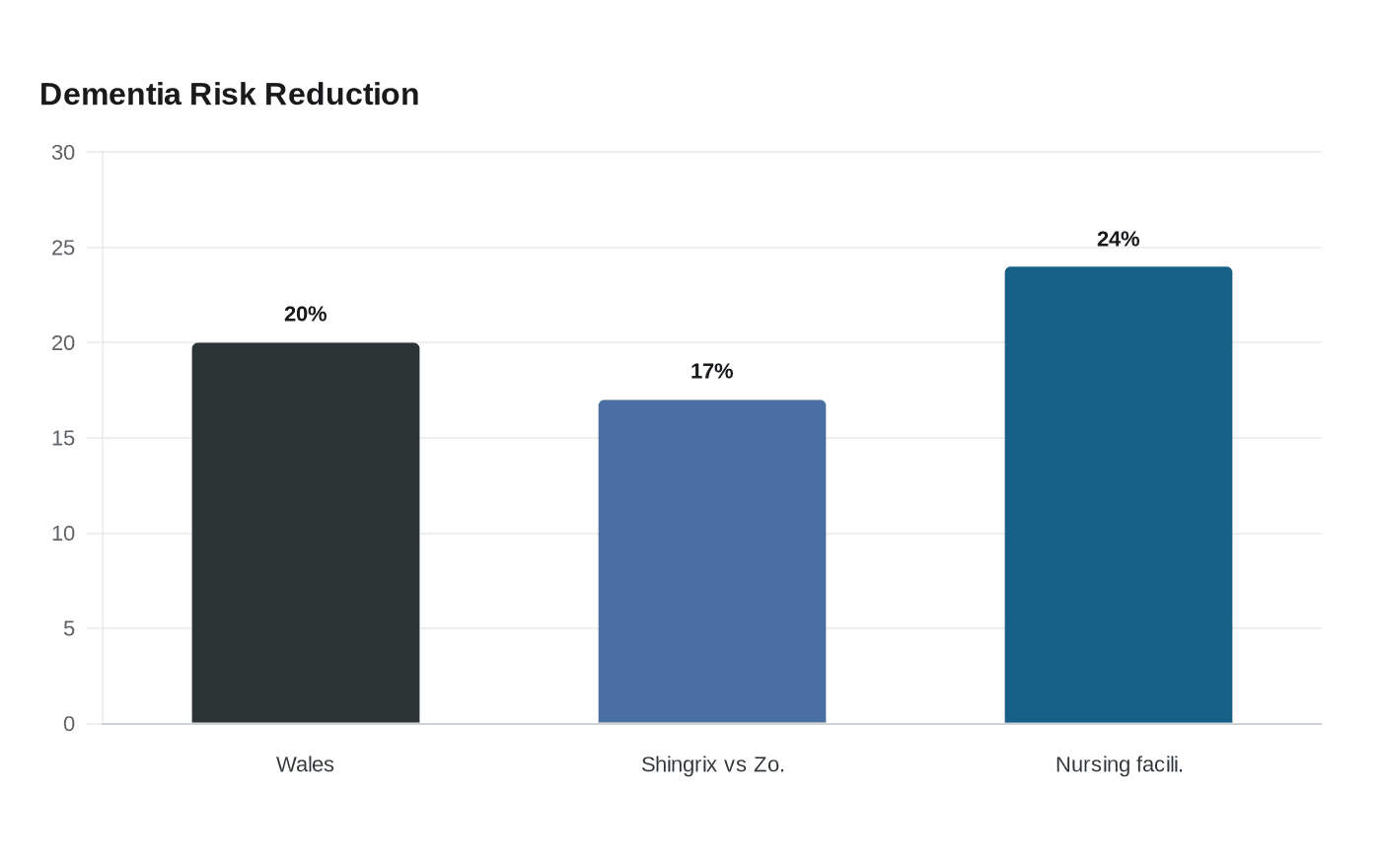
People who received the shingles vaccine in Wales were 20% less likely to develop dementia over the next seven years than those who did not. Large observational analyses, a natural experiment in Wales, and newer work in frailer older adults point in the same direction, though the evidence still points to association, not proof.
The current research does not justify calling the shingles vaccine a treatment for memory loss, but it does suggest that preventing varicella-zoster virus reactivation may be one of the more credible paths being tested in real-world populations.
What the newest studies found
A 2024 Nature Medicine study found the recombinant shingles vaccine, Shingrix, was associated with a lower risk of dementia than the older live-virus vaccine Zostavax. Shingrix was linked to a 17% lower dementia risk than Zostavax and a 23% to 27% lower risk than influenza and tetanus-diphtheria-pertussis vaccines. The gap translated into about 5 to 9 more months lived without dementia, with benefits seen in both sexes but greater in women.
A year later, Stanford-led research published in Nature used one of the strongest designs available for this question: a natural experiment in Wales. Because eligibility for the shingles vaccine depended on exact date of birth, people born before September 2, 1933 were ineligible, while those born on or after that date were eligible for at least one year. The vaccination program began on September 1, 2013, and about 47% of eligible 79-year-olds chose vaccination.
The Wales design is less vulnerable to healthy-vaccinee bias, the problem that healthier, more health-conscious people are often the ones most likely to get vaccinated. The authors called the finding evidence of a dementia-preventing or dementia-delaying effect from zoster vaccination that is less vulnerable to confounding.
Why scientists think this could be real
The leading theory is not that shingles vaccine directly targets Alzheimer’s disease itself, but that preventing viral reactivation may reduce one of the biological pressures that can push the brain toward degeneration. The findings support an emerging idea that viruses affecting the nervous system may contribute to dementia risk.

The immune response may also matter. AS01, the adjuvant in Shingrix, may be part of the explanation. That is a plausible clue, but still only a clue: the studies cannot show how Shingrix or Arexvy may protect against dementia and cannot rule out other factors.
The Wales study also widened the lens beyond prevention. In April 2025, the same analysis suggested the shingles vaccine may help people who already have dementia. Later Cell research found that vaccination reduced mild cognitive impairment and deaths due to dementia, suggesting that any effect could extend across the clinical course rather than only before symptoms begin.
What the data can, and cannot, prove
The studies use large populations and, in Wales, a policy cutoff that mimics random assignment more closely than ordinary observational research. Even so, none of the findings can prove causation on their own.
That means the vaccine may be associated with lower dementia risk because it helps biologically, but it could also reflect other differences between vaccinated and unvaccinated people that even sophisticated methods cannot fully erase. The direction of the findings is now consistent across several datasets, which strengthens the case for a real effect, yet the scientific standard for certainty has not been met.
The Brown University study, published in June 2026, extends the question to a frailer population often missing from early prevention research. Using Medicare and health records for more than 500,000 adults age 66 and older admitted to skilled nursing facilities from 2017 to 2022, researchers found that people vaccinated with Shingrix after entering a nursing facility had a 24% lower risk of being diagnosed with dementia over four years than those who were not vaccinated.
Nursing home residents face high medical complexity, more limited access to specialty care, and a heavier burden of dementia already in progress. The association persisted there, not just among healthy older adults with easy access to clinics.
What it should mean for vaccine decisions now
It should not change the basic shingles vaccine decision for most people, because Shingrix is already recommended in the United States for adults 50 and older as two doses separated by 2 to 6 months. The CDC also recommends two doses for adults 19 and older who are or will be immunodeficient or immunosuppressed. Zostavax is no longer available for use in the United States as of November 18, 2020.
The dementia findings may, however, add another reason to close gaps in shingles vaccination, especially among older adults and people at higher risk of complications from infection. Public health systems should treat this as an opportunity to improve uptake, not as permission to oversell a brain-health guarantee. The shot is recommended to prevent shingles and related complications, and it may also carry an added dementia benefit that is promising but unproven.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


