Perimenopause may be a critical window for heart-health prevention
Perimenopause is more than hot flashes: a 9,248-woman analysis links it to worse heart-health scores, giving clinicians a chance to screen earlier.
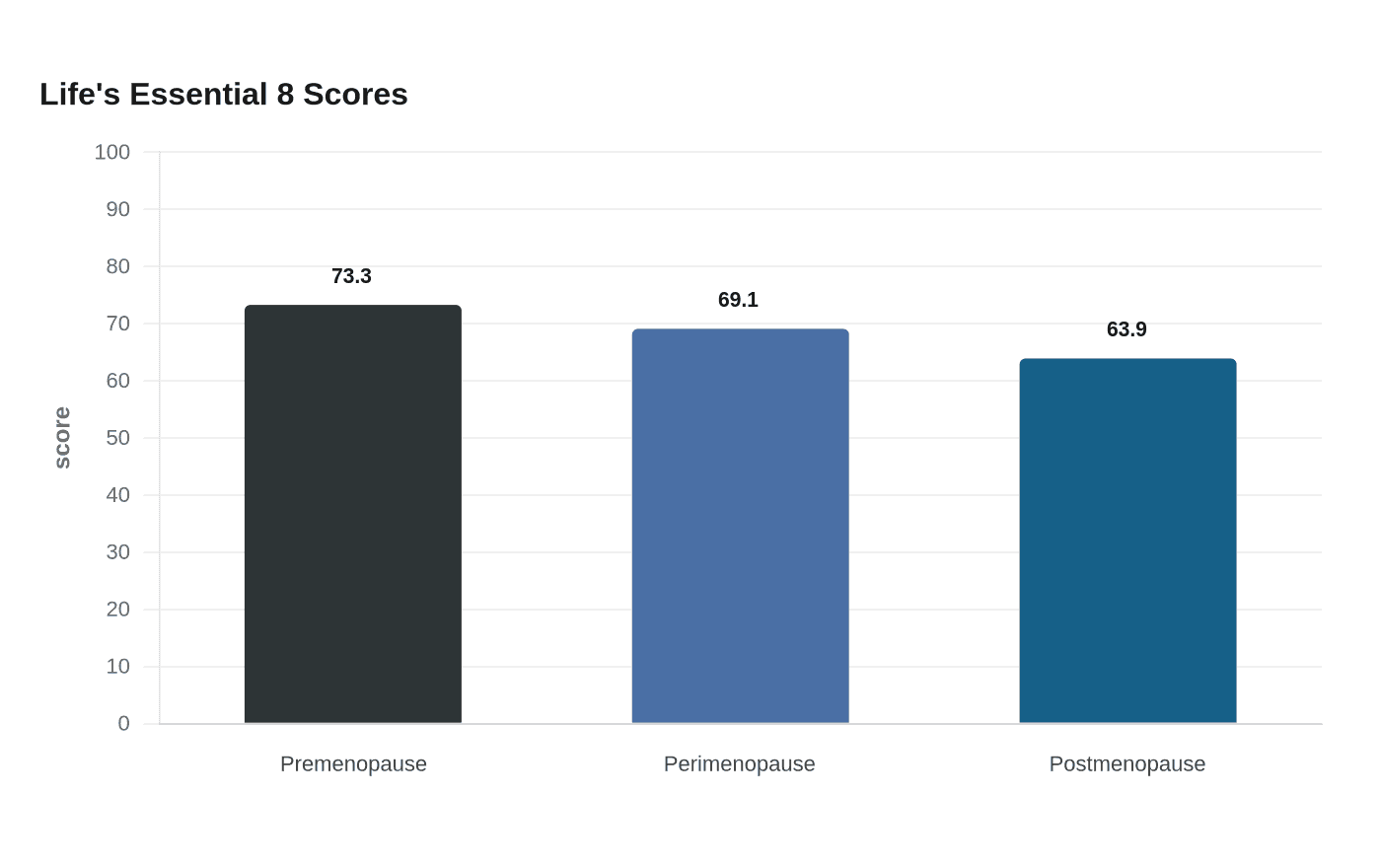
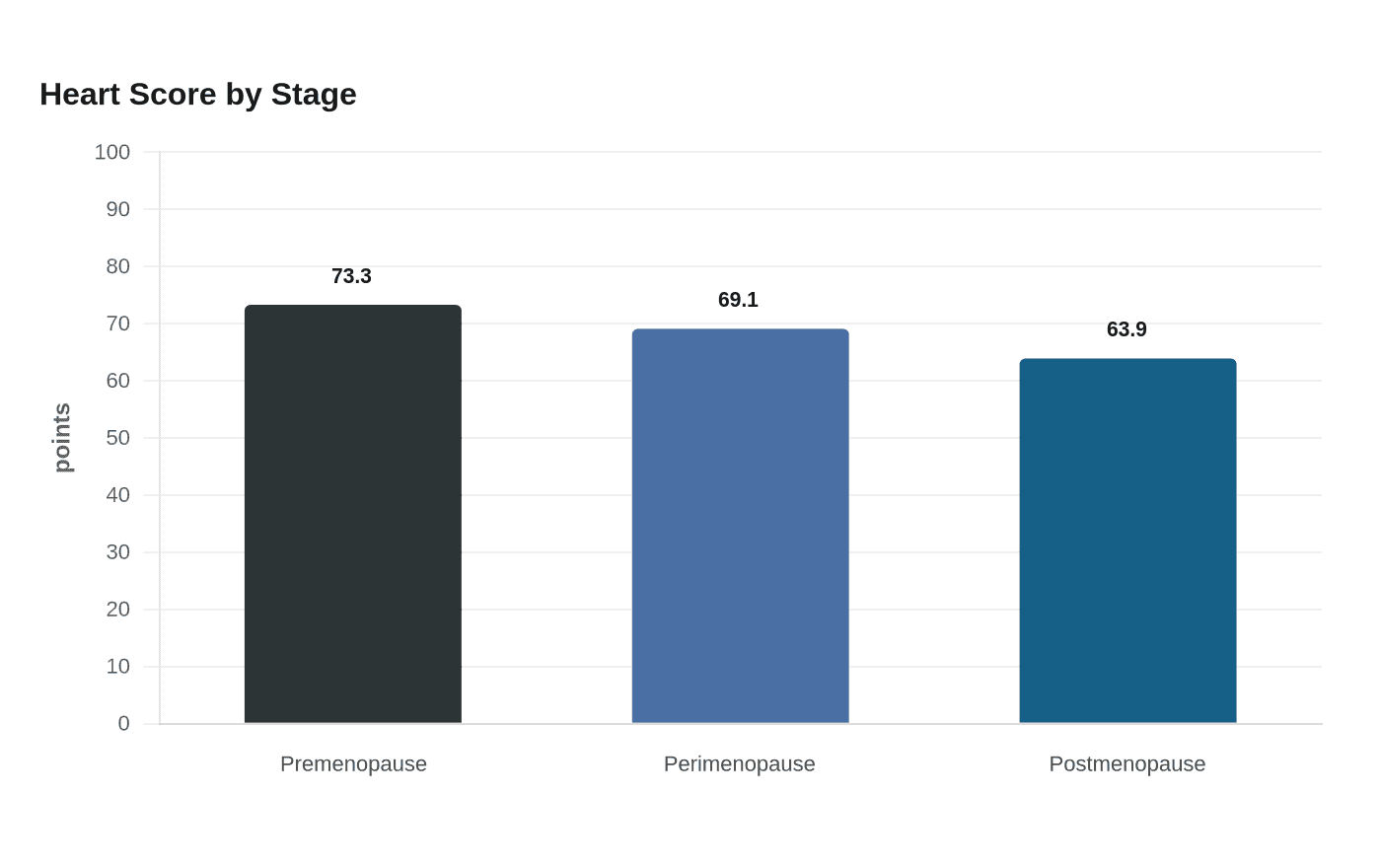
Median Life’s Essential 8 scores fell from 73.3 in premenopause to 69.1 in perimenopause and 63.9 in postmenopause in a new analysis in the Journal of the American Heart Association. The cardiovascular risk shift starts during this transition, before disease is obvious enough to force the issue.
Perimenopause is the missed-prevention window
The strongest case for acting now comes from a study that pulled National Health and Nutrition Examination Survey data from 2007 to 2020 and examined 9,248 women ages 18 to 80 who were not pregnant or breastfeeding and had no prior cardiovascular disease.
The adjusted findings are harder to ignore. Perimenopausal women had 1.92 times the odds of a poor overall Life’s Essential 8 score, 1.76 times the odds of a poor lipid score and 1.83 times the odds of a poor glucose score. In the same analysis, diet scored lowest across reproductive stages and sleep scored highest, while diet also declined over time.
Estrogen fluctuations help explain the shift. As hormone levels swing, cholesterol, insulin resistance, blood pressure and weight management can all become harder to control.
What the American Heart Association is asking clinicians to do
On May 13, 2026, the American Heart Association said women should be screened for cardiovascular risk factors throughout adulthood, but that perimenopause offers a “window of opportunity” to reassess risk and prompt lifestyle changes.
Garima Arora, a senior author on the JAHA paper, said midlife women should not wait until menopause to start checking blood pressure, cholesterol and blood sugar, and should talk with their care team about reproductive status and symptoms. In practice, menopause transition belongs in the same conversation as family history, blood pressure trends and lab work.
The AHA’s 2020 scientific statement in Circulation described the menopause transition as a critical window for early intervention strategies to reduce cardiovascular disease risk. It also noted that the 2011 women’s prevention guidelines did not include the then-available evidence on the transition.
The questions worth bringing to an appointment now
Midlife visits are more useful when they are specific. If you are in perimenopause, the most practical step is to turn vague unease into a short, direct checklist that covers both symptoms and risk markers.
- What is my current blood pressure, and how does it compare with past readings?
- When were my last cholesterol and glucose tests, and do they need repeating now?
- Given my family history, do I need a more detailed cardiovascular risk review?
- Has my exercise tolerance changed, and could that signal something beyond age or stress?
- Are my sleep changes, palpitations, migraines or cycle changes part of a menopause transition that should be documented?
- Should we talk about diet quality, physical activity, alcohol intake and weight change as part of prevention, not just symptom relief?
New fatigue on exertion, a drop in stamina, rising blood pressure or worsening lipids alongside cycle changes deserves a proper cardiovascular conversation rather than a shrug and a reassurance that it is all hormonal.
Beyond symptom relief: screening and risk stratification
A lot of midlife wellness marketing still frames perimenopause as a product category: supplement the sleep, calm the hot flushes, smooth the mood. Women’s health brands and telehealth platforms that only chase symptom suppression are missing the prevention opportunity that comes with screening, risk stratification and support for metabolic change.
The JAHA findings do not show a vague association at the margins. They show a measurable drop in overall cardiovascular health scores during the transition, with the sharpest penalties in lipid and glucose measures. Those are the same markers clinicians use to catch risk before it becomes disease.
The evidence has been building for decades
This is not a brand-new theory. A 1976 analysis from the Framingham Heart Study, published in the American Journal of Epidemiology, followed 1,686 women over nine biennial exams and found that natural menopause was associated with higher serum cholesterol levels. In that report, blood pressure and blood glucose did not significantly change, but the cholesterol signal was clear.
More recent reviews have continued to treat the menopause transition as a key prevention point, not just a reproductive milestone. Perimenopause may begin in the 30s or 40s, and premature menopause before age 40 is linked with a 40% higher lifetime risk of heart attacks. Black women were about three times more likely than white women to experience premature menopause.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


