3D-printed anatomical models improve surgical planning and patient outcomes
3D-printed anatomy is moving from novelty to operating-room tool, with 106 NHS cases showing better planning in 92.5% of responses and shorter surgery in 41.5%.

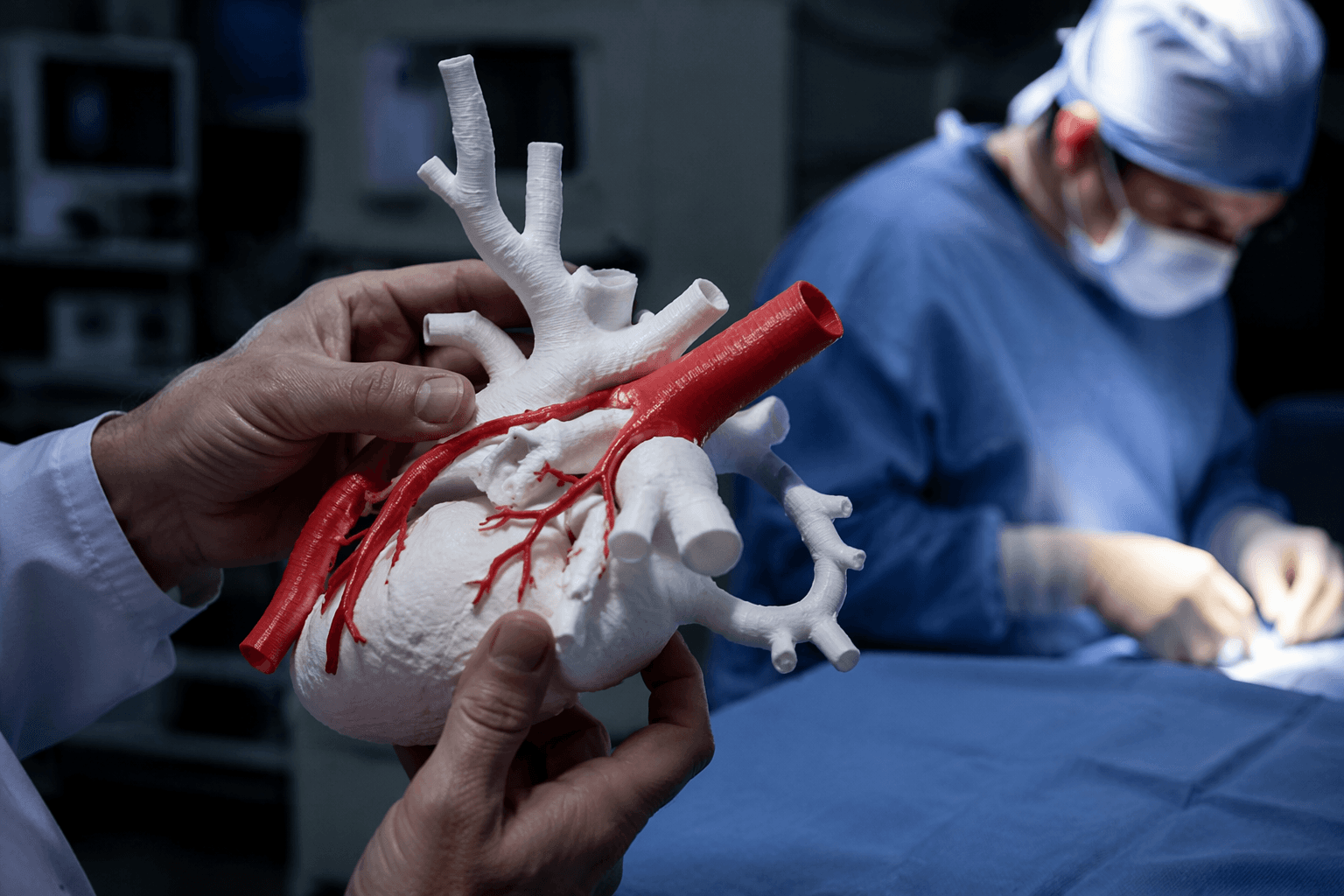
3D-printed anatomical models are paying off where surgeons feel it most: the exact fit of a case, the exact angle of an incision, and the exact risk hiding inside a scan. In complex procedures, the point is not just seeing anatomy on a screen. It is holding a patient-specific replica in hand, rehearsing the operation, and changing the plan before anyone scrubs in.
ENT surgeon Kyle VanKoevering, MD, used that approach early, first recreating and printing the head of a fetus with a potentially airway-obstructing facial mass to help decide whether a risky procedure would be needed during delivery. At Ohio State University, VanKoevering’s Medical Modeling, Materials and Manufacturing, or M4, Lab has kept using 3D printing to reduce risk and support clinical outcomes, and similar hospital programs are now running around the world. The models are being used to study individual anatomy before surgery, develop patient-specific implants and prostheses, and create life-like training cases for clinicians.
The clearest argument for the technology comes from the operating room data. A 2023 study of 106 complex surgical cases across NHS hospitals, involving 63 surgeons, found that 92.5% of responses said the 3D model was better than traditional 2D techniques for diagnosis and planning. The same study reported a 92.4% benefit for preoperative planning and a 92.6% improvement in surgeon-to-surgeon communication. It also found economic savings through better equipment selection in 54.4% of responses, while 41.5% reported reduced surgical time, a result the study linked to possible relief for surgical backlogs.
That same case-specific logic is driving use in the United States. At USF Health and Tampa General Hospital, physicians are printing replicas of organs such as aortas, kidneys, and jawbones so surgeons can rehearse procedures on exact physical copies of patient anatomy. Devid Zille, director of the 3D Medical Visualization and Printing Lab, said the models let surgeons “materialize what surgeons only see on screens.” Cardiologist Fadi Matar said the replicas help him anticipate coronary artery occlusion risk during valve replacement by showing how the coronary arteries relate to the valve being implanted.

The evidence is spreading beyond one specialty, too. Systematic reviews found that 3D printing-assisted surgery in pediatric upper and lower extremity cases reduced operating room time, blood loss, and radiation exposure, while work in foot and ankle fracture planning improved operation duration, intraoperative blood loss, fluoroscopy use, and ankle health scores. The barriers are still real, including high start-up costs, extra regulatory clearances, and the multidisciplinary training needed to run a hospital program. Implantable models face the strictest bar, with rigorous testing and FDA clearance required. But for the right case, the payoff is hard to miss: a scan becomes a physical rehearsal, and that can change the outcome before the first cut.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?