More Coffee Linked to Lower Mortality After Colorectal Cancer Diagnosis
The strongest coffee signal in colorectal cancer is showing up in stage III disease, but the data still point to association, not a prescription.

What the survival data actually says
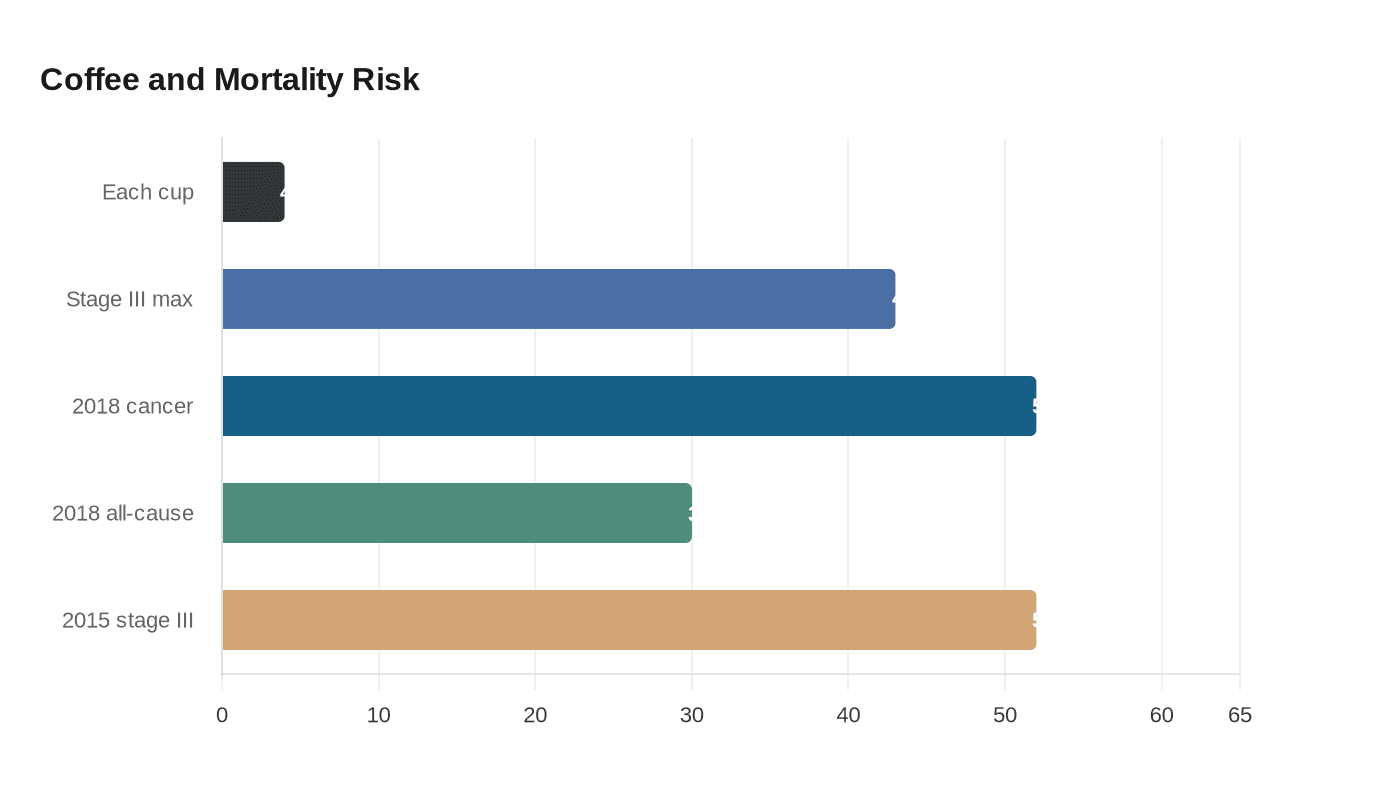
The number that jumps off the page is simple: in a newer analysis of 5,442 colorectal cancer patients, each additional daily cup of coffee was tied to a 4% lower risk of death after diagnosis, with stage III disease showing reductions as high as 43%. That is the kind of signal coffee people notice, not because it turns coffee into medicine, but because it keeps showing up in a disease where survival outcomes matter.
That pattern also fits the earlier Harvard-led work. In a 2018 Gastroenterology study, researchers followed 1,599 people diagnosed with stage I, II, or III colorectal cancer through the Nurses’ Health Study and the Health Professionals Follow-up Study. Patients who drank at least four cups of coffee a day had a 52% lower risk of colorectal-cancer-specific death and a 30% lower risk of death from any cause compared with nondrinkers, and the association was strongest in stage III disease.
A still earlier 2015 Journal of Clinical Oncology study in 953 stage III colon cancer patients from CALGB 89803 found the same kind of pattern. People drinking at least four cups per day had a 52% lower risk of recurrence or death than nondrinkers, which helps explain why stage III keeps emerging as the coffee-responsive subgroup in these datasets. This is not one isolated blip. It is a repeating result from overlapping but distinct patient groups, with Harvard T.H. Chan School of Public Health investigators including Mingyang Song, Shuji Ogino, and Edward L. Giovannucci, plus Jeffrey A. Meyerhardt and Charles S. Fuchs, repeatedly at the center of the analysis.
Why stage III keeps standing out
If you want the practical takeaway, this is it: the strongest coffee signal has not shown up evenly across all colorectal cancer stages. The 2018 Gastroenterology analysis said the association looked stronger in stage III than in stage I or II, and the 2015 CALGB 89803 data also focused on stage III colon cancer, where the recurrence-or-death reduction was most striking.
That matters because stage III disease is where treatment decisions and recurrence risk are already front and center. The repeated signal does not prove coffee is driving the difference, but it does suggest that the biology, treatment course, or patient characteristics in stage III may be where coffee’s association is most visible. In plain coffee-shop language, this is not a broad “everyone gets the same result” story. It is a “the stronger pattern keeps clustering in the more advanced stage” story.
Caffeinated, decaf, and what the cup is really telling us
One of the more useful details in the 2018 study is that the benefit was seen in both caffeinated and decaffeinated coffee. That is a big clue, because it pushes the conversation away from caffeine alone and toward the broader chemistry of coffee itself.
A review of coffee’s bioactive compounds has pointed to caffeine, caffeic acid, chlorogenic acids, and kahweol as candidate anti-cancer compounds. The fact that decaf also tracked with better survival makes the whole picture look more complicated than a simple stimulant story. It suggests there may be relevant compounds in the bean and brew beyond the caffeine hit people usually care about.
What these studies did not do is hand down a verdict on brewing method. They do not give coffee drinkers a clean answer on espresso versus drip versus French press, and they do not show that one extraction style changed survival outcomes. The evidence here is about intake and outcome, not about dialing in grind size, brew ratio, or water temperature.
What this does not prove
This is where the hard-nosed reading matters. All of these studies are observational, so they can show correlation, not proof that coffee itself improves survival. People who drink more coffee after a cancer diagnosis may differ in other ways, from overall health status to treatment tolerance to lifestyle habits that are hard to fully untangle.
That is exactly why Kimmie Ng of Dana-Farber Cancer Institute has kept the interpretation restrained in the 2021 JAMA Oncology discussion of these findings. The result is interesting, but it is not a basis to prescribe coffee as treatment. In other words, coffee may be a promising marker, and possibly a useful habit, but it is not a substitute for surgery, chemotherapy, surveillance, or the rest of standard colorectal cancer care.
What patients should actually do with this
The most evidence-minded move is not to start treating coffee like a supplement. It is to bring your real coffee habit into the oncology conversation in concrete terms: how many cups you drink, whether they are caffeinated or decaf, and whether coffee makes sleep, reflux, or stomach symptoms worse. That gives your care team something actionable to work with instead of a vague “I drink coffee sometimes.”
It also helps to keep the scale of the disease in mind. The National Cancer Institute’s SEER program estimated that 1,478,528 people were living with colorectal cancer in the United States in 2023, and about 3.9% of men and women will be diagnosed at some point in their lifetime. That is a large enough patient population that even a modest, repeated signal like this matters.
So the practical read is not “coffee cures cancer.” It is this: across multiple Harvard-linked analyses, higher coffee intake after colorectal cancer diagnosis has repeatedly lined up with lower mortality, most clearly in stage III disease, and the effect appears in both caffeinated and decaf coffee. That is enough to make coffee worth discussing with an oncologist, not enough to turn it into treatment on its own.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


