MBCT shows measurable cortical brain changes in depression study
A 66-woman randomized trial found MBCT plus usual care shifted EEG activity in major depression, lowering theta and raising upper alpha and low beta power.
Mindfulness-based cognitive therapy is getting a harder kind of test: not just whether people feel better, but whether the brain itself shows a measurable shift. In a new randomized study of women with major depressive disorder, MBCT added to treatment as usual was linked to lower theta power and higher upper alpha and low beta activity in cortical regions suggestive of insula and frontal cortex involvement. That makes this paper a reality check for the mindfulness field: encouraging, yes, but still a group-level signal rather than proof that brain-based change equals clinical cure.
What the study actually tested
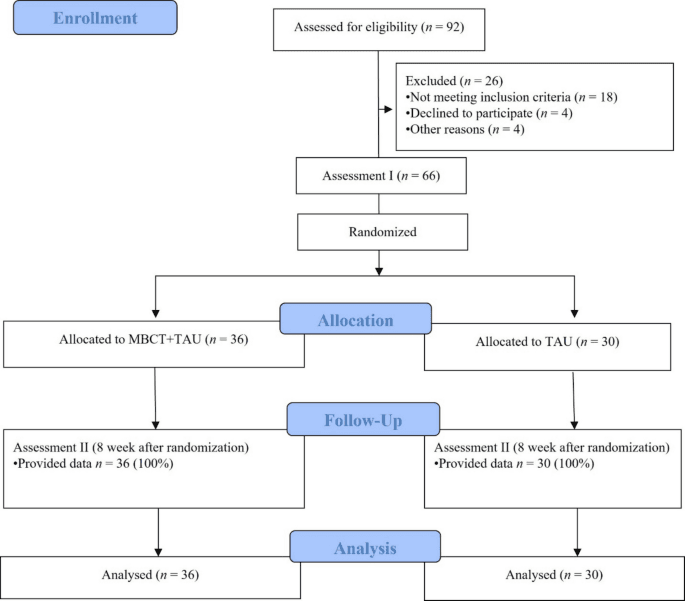
The new paper, published on June 10, 2026, set out to answer a very specific question: can MBCT change cortical electrical activity in people with major depressive disorder when it is added to standard care? The authors framed the problem around a familiar clinical limitation, namely that first-line pharmacotherapy for MDD is often not enough, then compared MBCT plus treatment as usual against treatment as usual alone. The trial enrolled 66 female participants with MDD, randomly assigning 36 to MBCT plus treatment as usual and 30 to treatment as usual alone, with stable-dose citalopram at 20 mg per day in both groups.
The design matters because it pushes mindfulness research beyond mood improvement alone. The primary endpoint was the Beck Depression Inventory-II, while the EEG work used power spectrum density from source localization with exact low-resolution electromagnetic tomography, or eLORETA. In other words, the study was built to ask whether symptom change and cortical electrical change could be observed side by side, not just whether participants said they felt calmer.
What changed on the EEG
The brain result was not vague. Compared with treatment as usual, the MBCT plus treatment as usual group showed significantly decreased theta power and significantly increased upper alpha and low beta power after treatment, in regions suggestive of insula and frontal cortex involvement, with corrected p values below 0.05. That is the kind of finding mindfulness researchers have been waiting for, because it gives the field a measurable electrophysiological pattern instead of relying only on self-report.

The clinical data moved in the same direction. Mean BDI-II scores fell from 28.08 to 11.58 in the MBCT plus treatment as usual group, and from 27.37 to 13.03 in the treatment as usual group, with a significant post-treatment group effect after adjustment for baseline scores. That does not mean the EEG change caused the symptom change, but it does show that the brain findings were not floating free of the clinical picture.
How this fits the wider MBCT record
This result lands inside a much longer MBCT story. The approach was originally developed by Zindel Segal, Mark Williams, and John Teasdale to help prevent relapse in recurrent depression, by teaching people to notice depressive thought patterns before they harden into the old spiral. A 2025 systematic review that brought together 87 studies said MBCT may induce neuroplastic changes and called for more work on long-term benefits and underlying neurobiological mechanisms.
The clinical evidence base is no longer small. A 2023 systematic review and meta-analysis included 13 studies with 1,159 participants, found that MBCT sessions typically lasted 1.5 to 2.5 hours over 8 weeks, and reported significant improvement in depression and suicidal ideation among people with MDD. For meditators, that matters because the new EEG paper is not arriving in a vacuum. It is extending an already crowded literature that has repeatedly suggested MBCT can help depressive symptoms when it is delivered as a structured program.
Why the older EEG work still matters
The 2026 paper also makes more sense alongside earlier neurophysiology studies. In a 2022 Frontiers in Psychiatry trial, researchers recruited 26 recurrent MDD patients with residual symptoms while they remained on antidepressants, then ran an 8-week MBCT intervention. After treatment, participants showed reduced depression, enhanced adaptive reflective rumination, and increased theta power and theta-band phase synchronization, with right occipital connections to right prefrontal, central, and parietal regions associated with reduced depression, and left parietal theta linked to better reflective rumination.
That earlier finding helps explain why the new paper is interesting even though it is not the last word. Across these studies, theta activity keeps showing up as a candidate mechanism, but the pattern is not a magic brainwave signature. It is a set of changes that seem to track with improved regulation, less depressive load, and in some cases less rumination.
What this does and does not prove
Here is the practical reality check for anyone tempted to treat a brain scan like a badge of clinical truth: measurable EEG change is promising, but it is not the same thing as universal effectiveness. This study supports the idea that MBCT can alter cortical electrical activity alongside symptom reduction in a specific group of women with MDD, yet it does not prove that every meditator will respond the same way, or that brain changes alone are enough to replace standard depression care. That is an inference from the study design and the broader review literature, not a claim that the paper itself settles the question.
For a mindfulness community used to hearing about calm, presence, and self-compassion, the useful takeaway is more concrete than inspirational: MBCT is increasingly being studied as a brain-based adjunct, especially when it is delivered in the classic 8-week format and paired with ongoing treatment. The strongest reading of this new paper is not that mindfulness has been “proved” by EEG, but that clinical mindfulness is getting closer to the kinds of objective markers psychiatry has been asking for all along.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?