Meditation changes pain processing differently in novice and long-term meditators
Beginners and long-term meditators do not seem to move pain the same way, with loving-kindness helping novices and attention-based states shifting experienced brains differently.
The pain signal did not budge, but the mind’s response did
Meditation did not act like a blunt painkiller in this study. When researchers measured brain responses to electric stimulation of the median nerve, they found that the raw, bottom-up sensory side of pain stayed largely the same, while the meaning and handling of pain shifted in more specific ways.
That difference matters because it draws a line between feeling the stimulus and processing it. The paper, received on May 17, 2025, accepted on February 22, 2026, and published online on April 10, 2026, makes a practical point that pain-focused meditators will recognize fast: the state you practice, and how long you have practiced, shape what changes most.
What the study tested
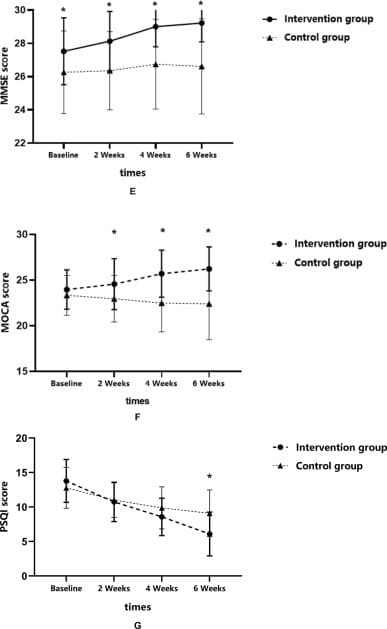
The researchers used EEG to track brain activity while participants were at rest and during three meditation styles: focused attention meditation, open monitoring meditation, and loving-kindness meditation. They compared short-term meditators with long-term meditators, which let them separate effects of the meditation state itself from effects of experience.
That design is the study’s real strength. Instead of treating meditation as one uniform practice, it asked which technique alters pain-related brain activity in which kind of practitioner. The answer was not that every style reduced pain in the same way, but that different states touched different layers of the pain experience.
Where beginners showed the clearest shift
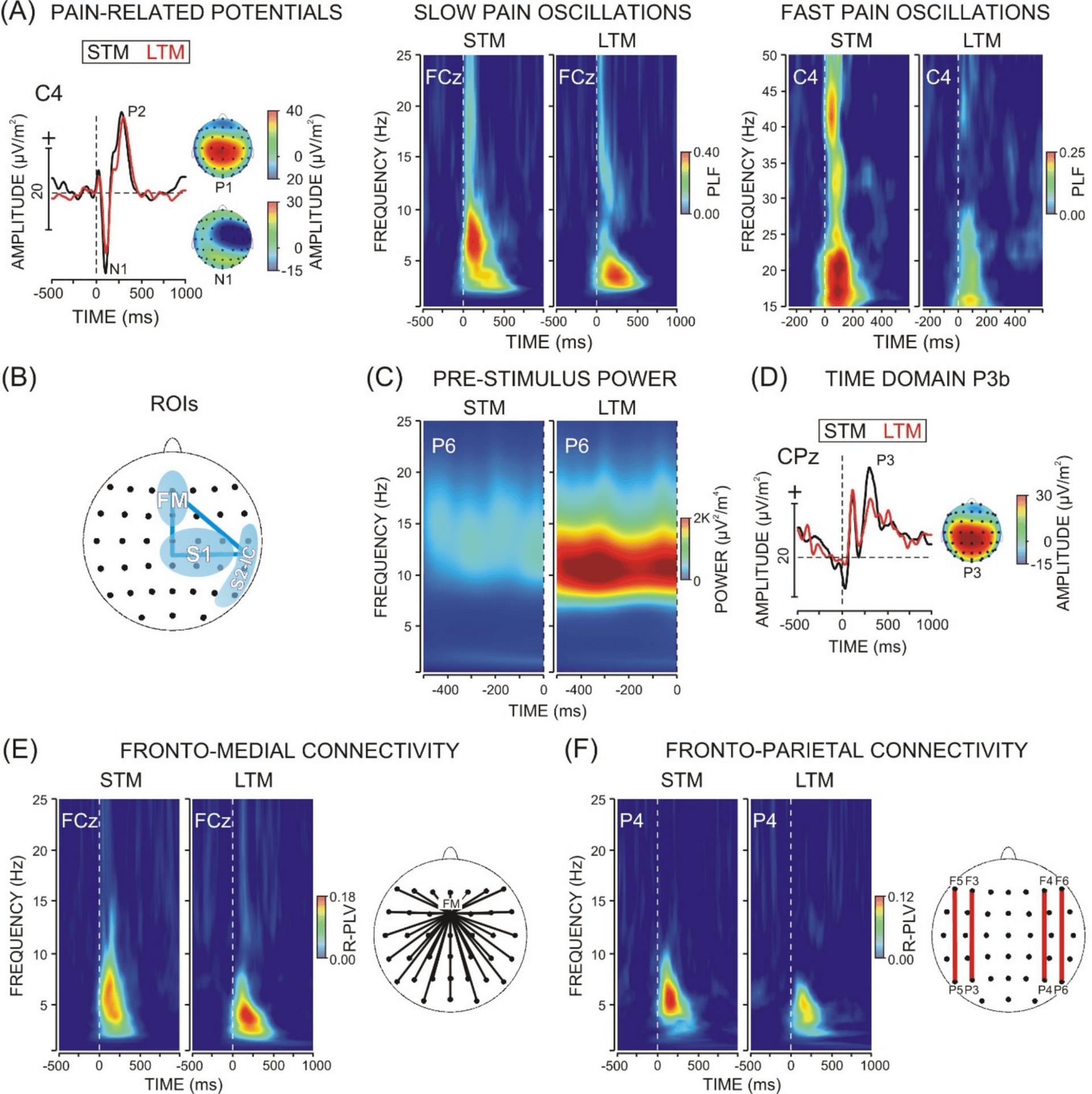
For short-term meditators, loving-kindness meditation stood out. The study found a significant decrease in connectedness of the fronto-medial theta-alpha network and a significant reduction of the P3b during loving-kindness practice. Those are not just technical details, they point to a change in how pain is being appraised and emotionally held in the moment.
In plain terms, the novice brain seemed to benefit most when the practice invited a positive emotional orientation. The effects were tied less to sensory filtering and more to how nociceptive signals were distributed and interpreted, especially when the meditation leaned into warmth, compassion, and benevolence. For someone new to mindfulness and trying to work with discomfort, that suggests a surprisingly practical entry point: a relational, heart-based practice may be easier to recruit than a purely attentional one.
Where long-term practitioners looked different
Long-term meditators showed their strongest changes during focused attention meditation and open monitoring meditation. The study reported a pre-stimulus alpha increase at somatosensory areas, along with modulations of fronto-medial and fronto-parietal theta-alpha synchronizations. Those shifts were associated with tighter functional segregation and fine-tuned involvement of cognitive-control and fronto-parietal attention networks.
That profile looks very different from the novice pattern. Instead of emotional soothing doing most of the work, experienced practitioners appeared to be using more refined internal attention control, with the brain organizing itself around how to observe, stabilize, and regulate the pain experience. In other words, the seasoned meditator’s edge was not a simpler or stronger signal of relief, but a more precise one.
What this means if you are using meditation for pain
The most useful takeaway is not that one technique is universally better. It is that meditation is not a one-size-fits-all tool for pain, and the mechanism seems to evolve with practice. If you are newer to mindfulness, loving-kindness may be the most immediately relevant state for pain work because it appears to change emotional appraisal and network connectivity rather than asking for advanced attentional skill.
If you have years of practice behind you, focused attention and open monitoring may be where the more measurable pain-related shifts show up. That makes sense clinically and in everyday life: a person trying to sleep through a flare, sit with post-workout soreness, or stay present during a medical procedure may need emotional buffering first, then attentional steadiness later. The study suggests teachers and therapists should match the practice to both experience level and the goal, whether that is emotional soothing, attentional stability, or a different relationship to pain.
How this fits the wider pain-and-mindfulness literature
This paper lands in a field that has already been pointing in the same direction. A 2021 systematic review of pain-related neural processes in expert and novice meditators selected 14 studies, including 5 EEG studies and 8 MRI or fMRI studies. Across that literature, both novice and expert meditators generally showed reduced pain ratings, but experts tended to show greater activity in somatosensory regions while novices showed reduced activity.
A 2020 review added another important piece: mindfulness lowers pain through brain processes that are distinct from placebo and vary across meditative training level. That review also underscored the scale of the problem, noting that chronic pain affects over 116 million Americans and about 1.5 billion people worldwide. That is why this field keeps drawing attention from the Centers for Disease Control and Prevention and from clinicians looking for nonpharmacologic options that can sit alongside other care.
The newer clinical evidence is moving in the same direction. A PubMed-indexed systematic review found that mindfulness meditation improves pain, depression symptoms, and quality of life in chronic pain, while still calling for larger, more rigorous randomized controlled trials. And a 2024 randomized clinical trial in veterans with chronic pain found that telehealth mindfulness-based interventions, both group-based and self-paced, improved pain-related function and biopsychosocial outcomes compared with usual care.
Where the study stops short
What this paper does not promise is just as important as what it does show. It does not say meditation erases the sensory input of pain. It does not suggest that a beginner can sit down and immediately get the same neural effects as a long-term practitioner. And it does not claim that one state, whether focused attention, open monitoring, or loving-kindness, is the universal answer for every kind of pain or every person.
Instead, it offers a more realistic map. Meditation appears to change pain processing most reliably in the layers above raw sensation, in appraisal, attention, and emotional orientation, and those layers shift as practice deepens. That is a more precise promise, and for people using mindfulness to work with pain, precision is often the difference between a nice idea and a practice that actually fits daily life.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?