U.S. Measles Surge Reaches 2,000 Cases, South Carolina Outbreak Grows
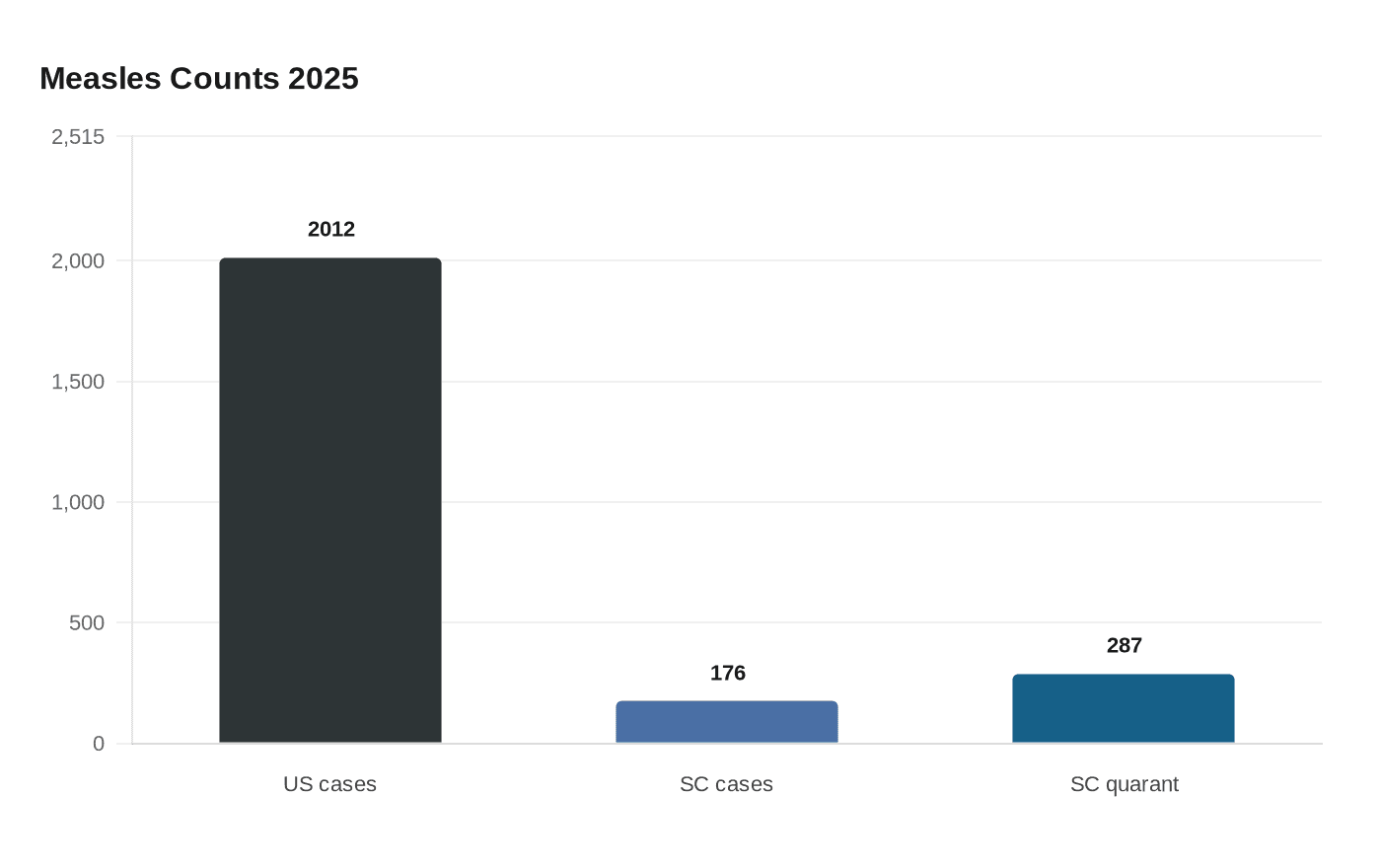
Measles has returned at levels not seen in more than 30 years, with the CDC logging 2,012 confirmed cases as of December 23, 2025, and a brewing outbreak in South Carolina reaching 176 cases by December 30. This article explains the scope of the national resurgence, the local dynamics in South Carolina, and what communities, health systems, and policymakers need to do to stop further spread and protect vulnerable people.

1. National Measles Surge
The United States has recorded a sharp resurgence of measles in 2025, with the Centers for Disease Control and Prevention logging 2,012 confirmed cases across multiple states as of December 23. That figure represents the highest total in more than 30 years and signals systemic gaps in vaccination coverage, public health capacity, and information environments that enable preventable disease to re-establish itself. Measles is extraordinarily contagious; a single case can infect many susceptible people, especially where vaccination rates fall below the herd immunity threshold. Public health implications include increased pressure on local health departments for case investigation and contact tracing, higher hospitalization risk among infants and immunocompromised people, and potential long-term complications such as encephalitis. Practically, stopping this trajectory requires rapid, equity-focused vaccination drives targeting under-immunized communities, strengthening school and childcare immunization policies, and ensuring accessible clinics with weekend and after-hours hours so working caregivers can get children vaccinated without losing pay. Policymakers should consider emergency funding to expand staff and laboratory capacity while addressing structural barriers to vaccination such as transportation, language access, and health insurance gaps that disproportionately affect low-income and marginalized communities.
2. South Carolina Outbreak
South Carolina’s outbreak escalated quickly at the end of December, with Reuters reporting on December 30 that the state had 176 confirmed cases and nearly 287 people in quarantine. That cluster highlights how a localized outbreak can amplify when containment measures are delayed or when populations with low coverage are geographically concentrated. The immediate community impact goes beyond case counts: quarantine orders disrupt livelihoods, schooling, and caregiving arrangements, and they place economic strain on families who lack paid sick leave or stable housing. For public health response, intensive contact tracing, rapid testing, and targeted vaccination clinics near affected neighborhoods are essential to interrupt transmission. Local health departments will need resources to support quarantined people with basic needs such as food, income replacement, and mental health resources to ensure compliance without imposing undue hardship. From a policy perspective, South Carolina’s situation underscores the need to revisit exemption policies for school immunization, invest in community-based outreach that builds trust rather than punishes, and coordinate with state and federal partners to deploy mobile vaccine units and culturally competent communication campaigns that address specific concerns in affected communities.
Public health, equity, and operational considerations Both the national surge and the South Carolina outbreak reveal overlapping failings: declining local vaccination coverage, uneven public health funding, and social conditions that make isolation and quarantine difficult for many families. Measles prevention is straightforward medically, the MMR vaccine is safe and effective, but the social determinants of health determine who gets protected. Communities with lower access to healthcare, crowded living conditions, or histories of medical mistrust are at higher risk. Response strategies must therefore pair clinical interventions with social supports: free and convenient vaccination, multilingual education led by trusted community figures, paid leave or direct financial assistance for those in quarantine, and partnerships with schools, faith organizations, and community health centers to reduce barriers. At the policy level, short-term emergency funding needs to be coupled with longer-term investments in the public health workforce, modernization of immunization information systems to identify coverage gaps in real time, and thoughtful reforms to school vaccine exemption rules that balance individual rights with community protection.
- Get vaccinated if you or your children are not up to date on MMR; check immunization records with your provider.
- Communities should push for mobile and pop-up clinics in under-vaccinated neighborhoods and ensure clinics offer flexible hours and no-cost vaccines.
- Employers and policymakers must institute paid leave or other supports so people can comply with quarantine without risking income.
- Local health departments need sustained funding for contact tracing and culturally competent outreach rather than one-time crisis grants.
Practical actions individuals and leaders can take now
Conclusion The 2025 measles surge is a reminder that vaccine-preventable diseases return when the social infrastructure that supports immunization and disease control weakens. The national tally of 2,012 cases and the South Carolina cluster of 176 cases with nearly 287 people quarantined are not isolated statistics; they are indicators of inequities and policy gaps that require both immediate action and long-term investment. Protecting children, frontline workers, and vulnerable adults will demand science-led strategies grounded in equity and compassion.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


