Healthcare partnerships emerge as a growth area for food banks
Healthcare is pulling food banks into the care continuum, and that means new referral, data, and coordination work for everyone from drivers to directors.
Healthcare is changing what food recovery work looks like
The next growth spurt for food banks may not come from bigger warehouses or more pantry shelves. It may come from hospitals and clinics, where food insecurity is increasingly treated as part of patient care.

That shift matters for A Simple Gesture because the job is no longer just collecting food. It is becoming the kind of logistics-and-trust operation that healthcare systems need when they start screening patients and sending people out with a food need attached.
Why hospitals are now part of the food bank conversation
The push is coming from both policy and evidence. The Center for Health Care Strategies says many states require health care provider organizations to screen patients for social risk factors and refer them to community-based services. The CDC has also described screening-and-referral programs as a way to connect patients with unmet health-related social needs to community resources.
At the same time, Feeding America’s evidence review makes the health case plain: food insecurity affects health across the lifespan and can raise chronic disease risk. That helps explain why food access is moving from the edge of the health system toward the center of care planning, especially for hospitals trying to reduce gaps after discharge and clinics trying to connect patients with practical support.
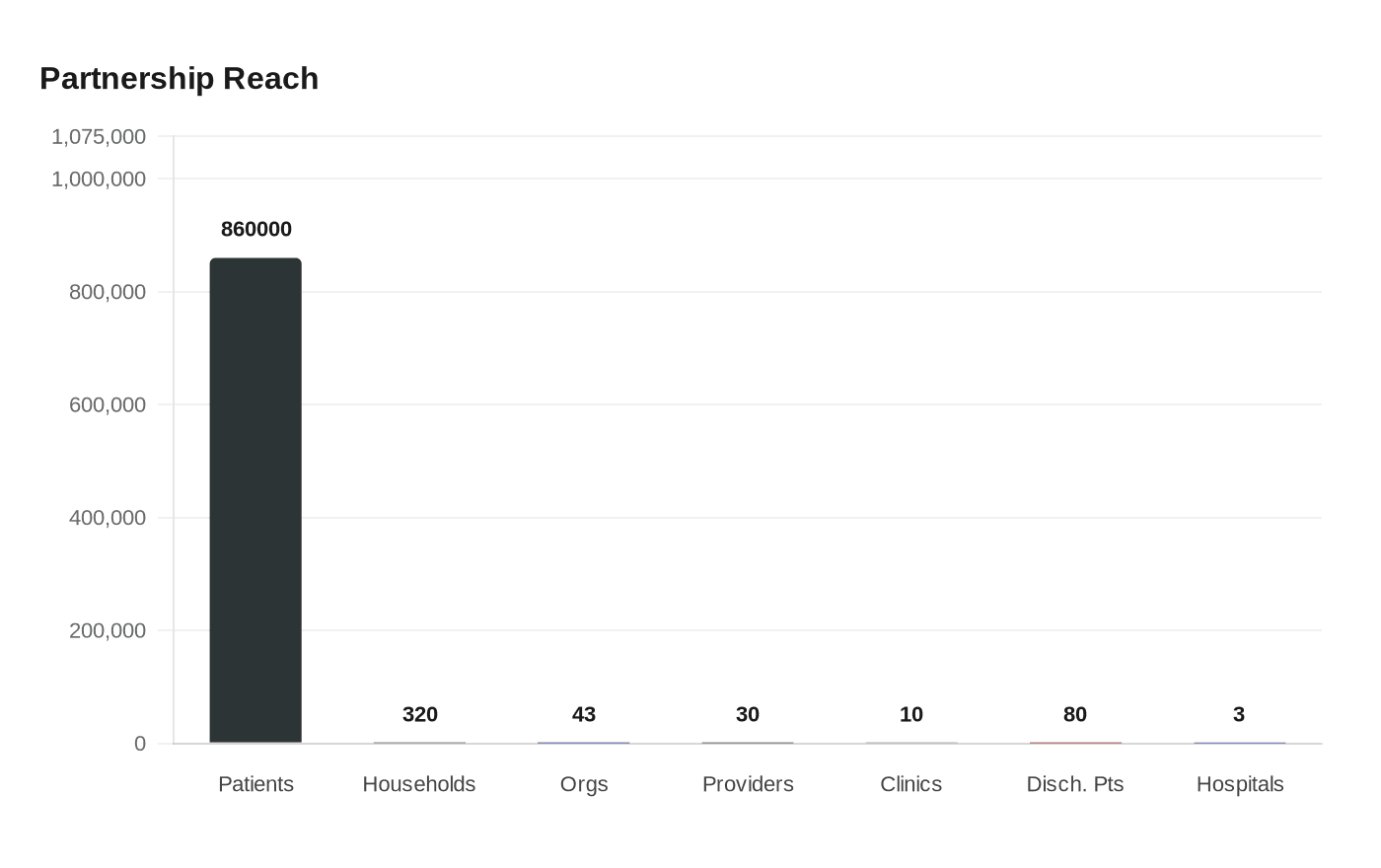
That national shift is already showing up in scale. Feeding America’s Food as Medicine initiative has involved more than 30 health care providers screening more than 860,000 patients for food insecurity during visits. Food Bank News also reported that Massachusetts reached a milestone when 43 community-based organizations, including many food banks, became Medicaid health care providers at the beginning of the year.
What this means for staffing and day-to-day work
For food banks, healthcare partnerships are not just another fundraising lane. They change the job mix. Staff need people who can manage referral pathways, keep schedules tight, coordinate with clinic staff, and document where food is going and why.
That means more than a warehouse team and a volunteer calendar. It means partnership managers, route coordinators, intake staff, and people who can translate between health system expectations and nonprofit reality. It also means leadership has to think about readiness and capacity, because the Center for Health Care Strategies’ toolkit advises food banks to assess both before building healthcare partnerships.
The work also gets more specific. Hospitals do not simply want to know that food exists somewhere in the community. They want reliable handoffs, clear accountability, and food services that fit the people they serve. The CHCS toolkit says culturally inclusive food services should be part of the model, which is a reminder that a successful partnership is about fit, not just volume.
What the model looks like on the ground
Long Island Cares offers a useful picture of how this plays out in practice. The food bank has built partnerships with the three main hospitals on Long Island, and one of those arrangements includes a mobile pantry that delivers food twice a week to about 80 discharged patients who lack support at home.
That same partnership also sends emergency food bags to emergency rooms and pediatric offices and runs monthly nutrition workshops. In workplace terms, this is a very different operation from a standard donation pickup. It requires scheduled delivery, close coordination with hospital staff, and enough consistency that clinicians can trust the food bank as part of the patient support network.
Chester County Food Bank in Pennsylvania shows another version of the same trend. It is working with ten community healthcare clinics to give patients payment cards that can be redeemed for fruits and vegetables at the food bank’s mobile market. The cards average about $400, are currently used by roughly 320 households, and can be used throughout the growing season from June to October, with plans to expand further.
That matters because it turns food access into a more intentional care pathway. Instead of a one-time referral, the system connects clinic visits to a specific nutrition resource with a defined redemption process. For staff, that means more tracking, more partner education, and more coordination across food access, scheduling, and patient outreach.
Why A Simple Gesture is already in the middle of this shift
A Simple Gesture already operates in the kind of community infrastructure that healthcare partners are looking for. Its Guilford County model includes Green Bag donations, food recovery, and SHARE school refrigerators, and the organization says it rescues edible food from businesses and delivers it to local nonprofits.
That is a big advantage, because health systems want partners who know how to move food reliably through a network, not just one who can accept a drop-off. A Simple Gesture-Guilford County says it has followed a template established in 2011 and was set up as a 501(c)(3) nonprofit in 2015, which gives it the kind of organizational staying power that hospitals and clinics tend to look for when they build long-term referral relationships.
The organization’s partnerships with dozens of local pantries also matter. Food banks and clinics may be the public face of this trend, but the real work still lands in neighborhood distribution points, school refrigerators, and recovery routes. Those are the places where a household’s need becomes visible, and where a simple donation pipeline can actually turn into a response.
What staff and volunteers will need next
For A Simple Gesture, the big lesson is that healthcare partnerships reward operational discipline. Volunteers and coordinators will need to be even more precise about pickup timing, route reliability, partner communication, and the handoff between recovered food and the nonprofits that receive it.
A few practical shifts stand out:
- Build stronger referral workflows, so a hospital or clinic knows exactly who to contact and what happens next.
- Tighten route coordination, especially when deliveries have to align with discharge planning or clinic hours.
- Make partner reporting simple and consistent, so local health systems can see that food reached the right place.
- Keep culturally inclusive food options in mind, since the healthcare side is increasingly thinking about nutrition, not just calories.
- Train staff and volunteers to think in cross-sector terms, where the job is not only moving food but supporting health outcomes.
The broader message is straightforward. Food recovery is no longer just a charitable supply chain. It is becoming part of community health infrastructure, and the organizations that thrive will be the ones that can handle both the human side of hunger relief and the operational demands of healthcare collaboration.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


