Mammogram guidelines shift as experts debate when screening should start
Mammogram advice has converged on age 40 for many women, but the right start date still depends on risk, breast density and symptoms. Knowing which guideline applies can prevent both missed cancers and unnecessary testing.
Why mammogram advice still feels unsettled
Mammogram screening has become a moving target because the major guideline groups are answering slightly different questions. Some recommendations are built for women at average risk and with no possible cancer symptoms, while others try to set a broader national standard for earlier detection. That split is why a 40-year-old can hear one expert say to start now, while another still frames the choice as something to discuss.
The stakes are not abstract. The American Cancer Society says about 1 in 8 women in the United States will develop invasive breast cancer in her lifetime, about half of women diagnosed are 62 or younger, and breast cancer remains the most commonly diagnosed cancer in U.S. women and the second-leading cause of cancer death after lung cancer. In that context, even small shifts in screening policy can affect how many cancers are found early, how many are missed, and how many women are sent for extra tests they may not need.
What the major guidelines now say
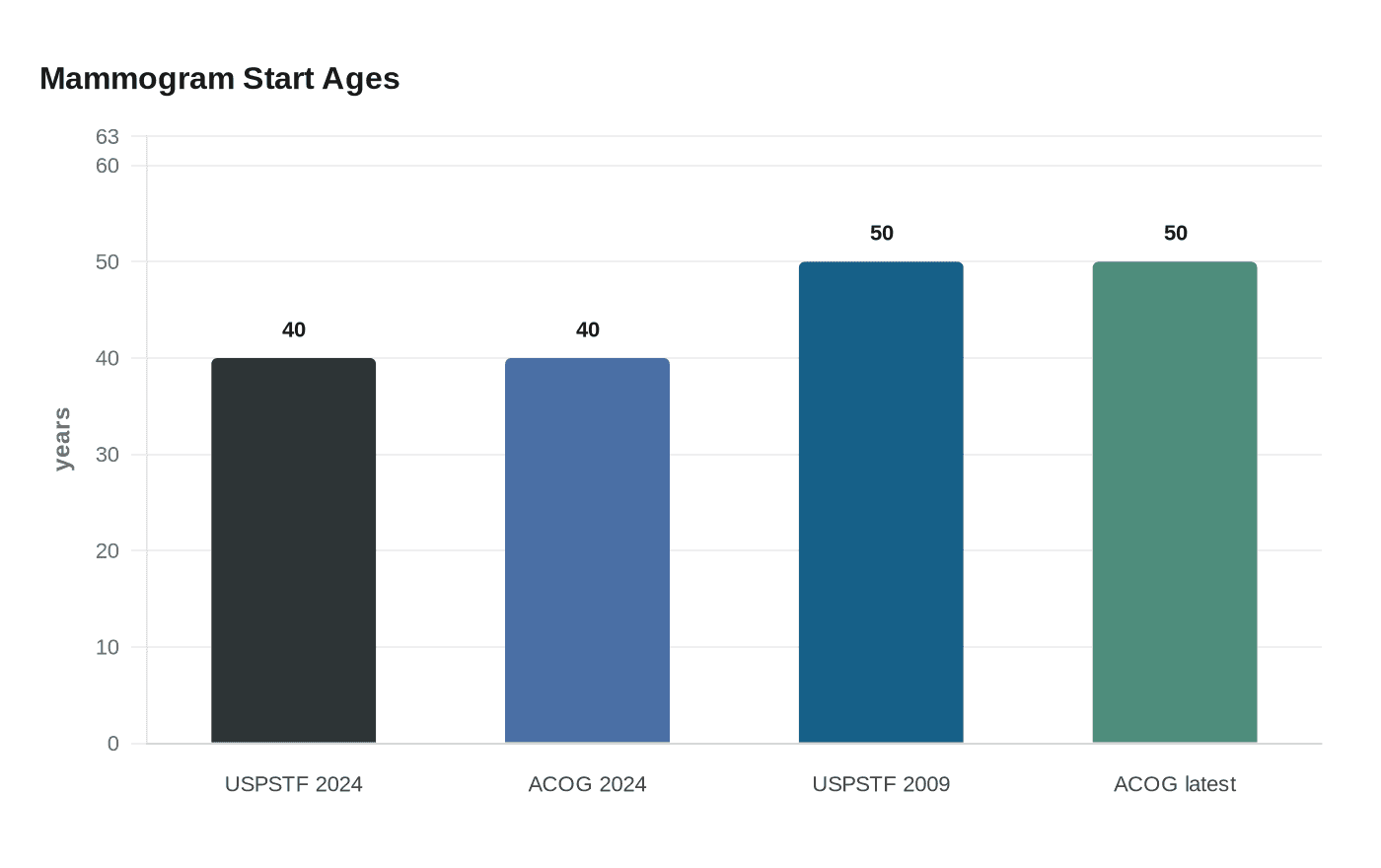
The U.S. Preventive Services Task Force updated its final recommendation on April 30, 2024, advising biennial screening mammography for women ages 40 to 74. That was a clear change from the group’s earlier approach, which had recommended starting at 50 and making individualized decisions in the 40s. The Task Force also says evidence is insufficient to judge the benefits and harms of screening mammography for women 75 and older.
The American College of Obstetricians and Gynecologists went even further in October 2024, recommending that average-risk women begin screening mammography at age 40 and continue every one or two years through shared decision-making with their clinicians. ACOG also says women who have not started in their 40s should begin no later than age 50. The American Cancer Society, meanwhile, says regular screening mammography is the most reliable way to find breast cancer early for women at average risk.
Those differences may sound small, but in practice they shape who gets screened, how often, and with how much urgency. Biennial screening means every two years, which is easier to remember and less burdensome, while annual or one-to-two-year screening gives clinicians room to tailor the schedule to a woman’s age, family history, breast density and comfort with uncertainty.
Why the conflict exists
Part of the confusion comes from history. The Task Force’s 2009 guidance recommended biennial screening for women ages 50 to 74 and said the decision to start before 50 should be individualized. Its 2016 guidance also fed the long-running debate over whether the 40s should be treated as a routine start point or a shared decision. Once one influential group moved toward 40, others were forced to clarify whether they agreed, and how strongly.
The deeper reason is that screening is always a balance. Earlier mammography can catch cancer sooner, which can matter because some tumors grow quickly and outcomes are often better when disease is found at an earlier stage. But mammography can also produce false positives, which can cause emotional distress and lead to extra imaging or biopsy. For many women, the question is not whether screening matters, but how much false alarm risk they are willing to accept in exchange for earlier detection.
Average-risk women versus women who need a different conversation
The newest screening recommendations are aimed at women at average risk. That usually means women without a known major inherited cancer syndrome, without a personal history of breast cancer, and without symptoms that could suggest an active problem. Those symptoms, such as a new lump, nipple discharge or skin change, move the discussion away from routine screening and into diagnostic evaluation.
Women at higher risk often need a different plan than the average-risk guidelines describe. That group can include women with a strong family history, known inherited mutations, prior chest radiation or other factors that raise the odds enough to justify earlier or more intensive surveillance. For them, the question is not simply whether to start at 40, but whether mammography should be paired with other imaging or begin even earlier.
That distinction matters because a single age-based rule can be misleading. A woman with no special risk factors may reasonably follow the age-40 guidance and still decide whether to screen annually or every two years. A woman with a substantial family history may need a risk assessment first, because her plan may involve more than the standard mammogram schedule.
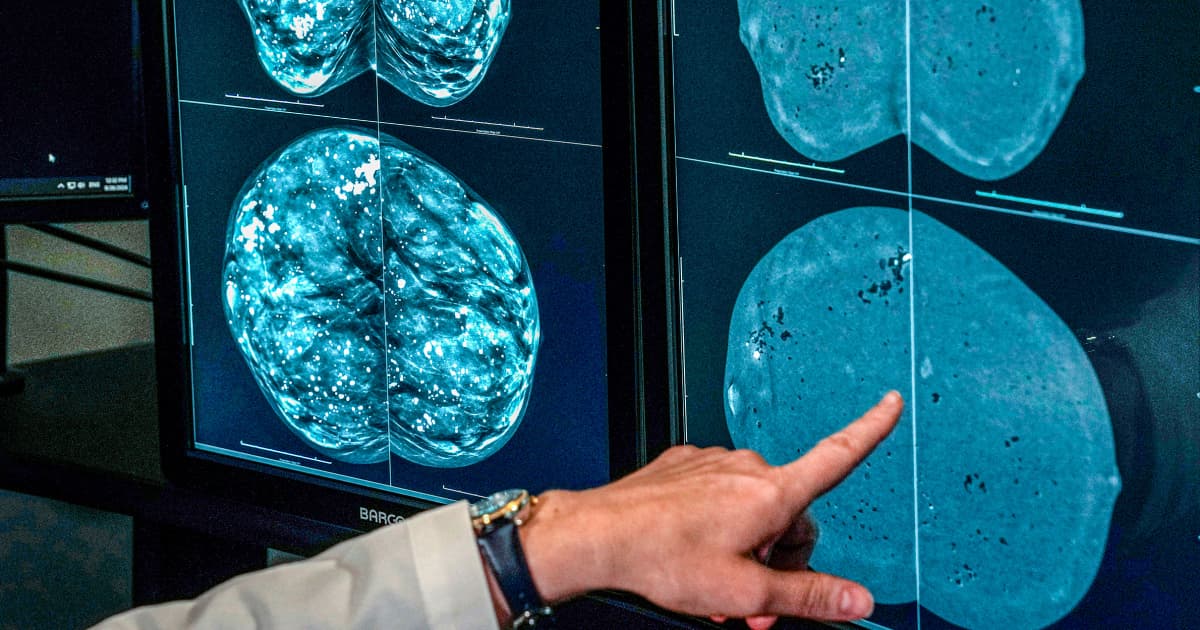
Dense breasts add another layer of uncertainty
The Food and Drug Administration’s mammography notification rule took effect on September 10, 2024, requiring facilities to tell patients about breast density. Dense tissue matters for two reasons: it can make cancer harder to spot on a mammogram, and it also raises breast cancer risk. That means a woman can have a negative mammogram and still leave with unresolved questions if her breasts are dense.
Even here, the evidence is not simple. The Task Force says evidence is insufficient to evaluate supplemental ultrasound or MRI screening for women with dense breasts after a negative mammogram. In practical terms, that does not mean those tests never help; it means the evidence base has not settled the tradeoffs well enough for a universal recommendation. Extra imaging can find additional cancers, but it can also drive more false positives, more callbacks and more biopsies.
For patients, dense-breast notifications are a prompt to ask whether density changes the screening plan. In some cases, density is one factor among many. In others, it is enough to justify a more detailed conversation about whether MRI, ultrasound or a different screening interval makes sense.
Why race and age 40 remain central to the debate
The screening debate is also about equity. Centers for Disease Control and Prevention data show breast cancer mortality disparities have remained consistent over the past two decades. A 2021 CISNET analysis found that if Black women began biennial mammography at 40, breast cancer deaths could be reduced by 57 percent compared with starting 10 years later.
That finding helps explain why some experts and advocates argue that age-40 screening is especially important for Black women and other populations that face worse outcomes. The issue is not only biology, but also access, timing and the cumulative effect of delayed detection. When mortality gaps persist even as screening technology improves, starting earlier can become a public health strategy as much as a personal choice.
Questions to ask before you schedule your next mammogram
- Am I truly average risk, or do my family history, prior biopsies, genetic factors or symptoms put me in a higher-risk category?
- How does my breast density affect the limits of a standard mammogram?
- Should I screen every year or every two years, given my age and risk profile?
- If my mammogram is negative but my breasts are dense, would additional ultrasound or MRI be helpful, or would it mostly add false alarms?
- If I am in my 40s and have not started screening, why would one guideline suggest now while another emphasizes shared decision-making?
The clearest takeaway is that the age-40 shift is real, but it is not a one-size-fits-all command. Screening works best when the schedule matches the woman, not just the calendar, and the most useful mammogram advice is the kind that accounts for risk, density and the tradeoffs between earlier detection and unnecessary follow-up.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


