Medicus Pharma Submits Optimized Phase 2 Study Design for BPH Drug Teverelix
No drug is currently approved to prevent acute urinary retention from recurring. Medicus Pharma filed a refined Phase 2 protocol for teverelix with the FDA to target that gap.
No currently approved pharmacological therapy prevents acute urinary retention from recurring once a man has survived an episode, a gap Medicus Pharma is explicitly targeting with teverelix, its investigational gonadotropin-releasing hormone antagonist. The Philadelphia-based biotech filed a refined Phase 2 protocol with the U.S. Food and Drug Administration on April 6, advancing an existing Investigational New Drug application rather than opening a new regulatory dossier.
The submission is a study-design milestone, not a demonstration of efficacy. Protocol ANT-2111-02 still requires FDA review before a single patient can be enrolled, and the agency's written feedback will determine whether the design proceeds as submitted or requires further modification.
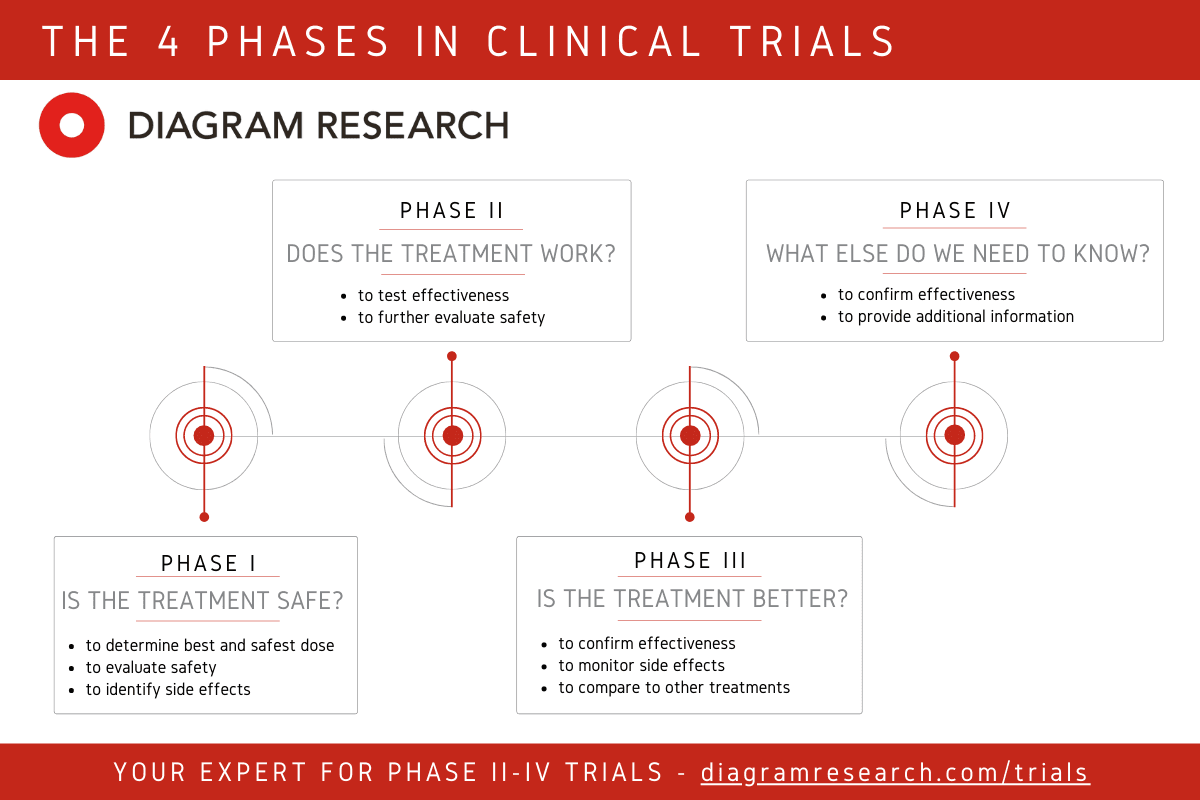
What Medicus has put before the FDA is a randomized, double-blind, single-dose, four-arm trial targeting approximately 126 men across sites in the United States and Europe. The design tests two formulations of teverelix: 90 milligrams delivered intramuscularly and 120 milligrams delivered subcutaneously, each compared against a matched placebo. All participants receive a single injection on Day 1 and continue on standard-of-care background therapy. The primary endpoint is pharmacodynamic: total prostate volume reduction, a measurable signal of androgen suppression that would indicate teverelix is doing what its mechanism predicts.
The study design was developed under the direction of Steven A. Kaplan, M.D., FACS, a urologist Medicus described as a globally recognized leader in men's health, who is expected to serve as principal investigator. The choice to anchor the primary endpoint in prostate volume rather than a harder clinical outcome reflects a deliberate proof-of-concept strategy, prioritizing a detectable pharmacodynamic signal in a smaller patient population before committing to a larger, longer outcomes study.
The clinical rationale rests on a genuine care gap. Acute urinary retention is a sudden inability to void that sends men to emergency departments for catheterization, an invasive procedure that carries infection risk and significant discomfort. In men with benign prostatic hyperplasia, the condition recurs at troubling rates; historical data show surgical intervention followed the initial episode in only a minority of patients in recent years, leaving a substantial population cycling through catheterization and medical management with no drug specifically approved to interrupt that cycle. Medicus estimates the addressable market at approximately $2 billion. Chief Medical Officer Dr. Faisal Mehmud has cited the absence of any approved preventive pharmacotherapy as the core competitive opportunity for teverelix.
For investors assessing the announcement, the distinction between a protocol submission and a proof of clinical benefit matters significantly. An IND amendment confirms the FDA has received the document; it does not signal agency endorsement of the design, projected enrollment timelines, or likelihood of success. What the FDA's feedback will reveal is whether the agency accepts prostate volume reduction as a sufficient Phase 2 endpoint, whether the dosing rationale for the two formulation arms is adequately supported, and whether site activation across two continents is operationally realistic given Medicus's reported year-end 2025 cash position of $8.7 million.
If ANT-2111-02 eventually enrolls and meets its primary endpoint, the result would still represent a mechanistic signal, not a registration-ready filing. Changing emergency department and urology practice would require demonstrating, in a larger pivotal cohort, that prostate volume reduction translates into fewer catheterizations, fewer hospitalizations, and durable symptom relief. The Phase 2 now before the FDA is the required step before that evidence can be generated.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


