Nuclear medicine faces isotope bottlenecks as aging reactors strain supply
A handful of aging reactors quietly powers most Tc-99m scans, and one pipe problem in Petten showed how fast that narrow supply chain can shake hospitals.

The narrow pipe behind a routine scan
Technetium-99m is the isotope that keeps modern nuclear medicine humming. More than 40 million diagnostic procedures a year depend on it, and the OECD Nuclear Energy Agency says it shows up in 85% of diagnostic nuclear medicine scans worldwide, covering roughly 30 million patient examinations each year. That is an enormous clinical footprint for a material most patients never see, and it is exactly why the supply chain matters so much.
The catch is that Tc-99m is not a material you can warehouse and forget about. Its physical half-life is about six hours, which means it has to be produced near the place and time it is used, then moved through a generator system built around its parent isotope, molybdenum-99. Mo-99 itself lasts only about 66 hours, so the whole chain runs on continuous output, fast processing, and tightly choreographed logistics rather than storage cushion.
Why the system is fragile by design
That short clock changes everything. When a product decays this quickly, every delay compounds: reactor downtime, processing delays, transport hiccups, and weekend scheduling all become part of the medicine. The OECD and IAEA have both treated this as a structural problem for years, not a temporary inconvenience, because the chain cannot absorb much slack.
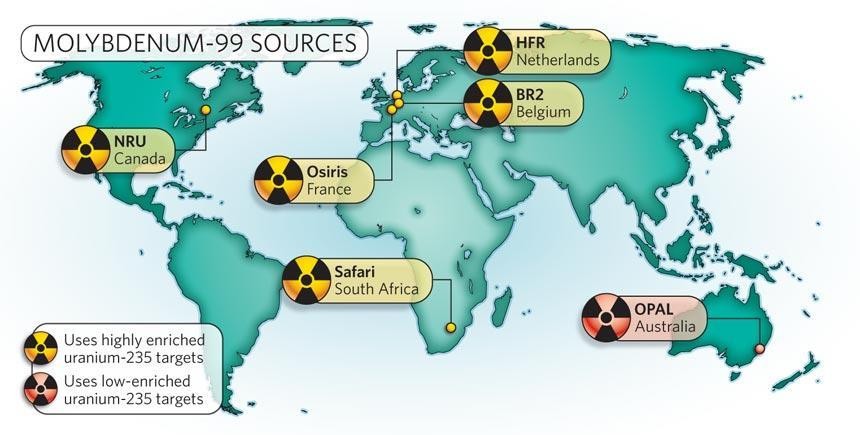
The deeper issue is that the production system was never built as a pure medical factory. OECD countries still rely on a relatively small number of multipurpose, aging research reactors to supply nearly all of the world’s demand for Mo-99. That concentration creates single points of failure, and it means maintenance windows, unexpected outages, and capacity limits can ripple straight into hospitals. In this market, scarcity is not mainly about demand running hot. It is about infrastructure running thin.

When one reactor problem becomes everyone’s problem
A clean example landed in October 2024, when a pipe deformation at the High Flux Reactor in Petten, Netherlands, raised concerns about Mo-99 shortages. The American Society of Nuclear Cardiology said the issue needed an immediate fix rather than the planned repair scheduled for December 2024, which tells you how little room there is to maneuver when the isotope pipeline is already tight.
That Petten episode matters because it shows how fast a technical issue becomes a medical one. If a reactor or processing line slips, the effect is not abstract. It shows up as delayed doses, rescheduled scans, and pressure on every downstream link that depends on Mo-99 arriving on time and in usable quantity. The fragility is not just in the reactor core. It is in the processing line, the handoff to the generator system, and the logistics chain that has to keep pace with a six-hour isotope.
The United States is trying to diversify the chain
U.S. policy has tried to solve part of the problem through domestic production. The U.S. Department of Energy’s National Nuclear Security Administration says the American Medical Isotopes Production Act of 2012 directed it to establish domestic supplies of Mo-99 without using highly enriched uranium. That matters for more than one reason: it is about resilience, but it is also about nonproliferation and reactor policy.
The NNSA says its program has supported seven different U.S. companies over the years, which is the right idea for a brittle supply chain. Spread the risk, back multiple pathways, and do not bet the whole country on a single producer or reactor. The broader lesson is obvious to anyone who has watched a difficult build or a temperamental system in any branch of nuclear work: redundancy is not waste, it is insurance against the moment the main line goes down.
What resilience looks like now
The OECD and IAEA have both been blunt that interruptions in Mo-99 supply pushed governments and international agencies toward both short- and long-term solutions. That is why this story is bigger than one isotope. It is really about how the medical side of the nuclear industry is being forced to modernize the same way any fragile technical system eventually has to: by building more routes, more capacity, and more tolerance for failure.
The OECD has also kept the conversation moving beyond Mo-99 and Tc-99m into newer therapeutic radioisotopes such as lutetium-177 and actinium-225. That is an important shift, because it widens the definition of supply resilience from simply keeping scans running to building a broader radioisotope ecosystem that can support diagnosis and treatment alike. If the sector gets this right, it will not just protect hospitals from shortages. It will make the whole nuclear materials chain less dependent on a handful of aging reactors and a few unforgiving hours of decay.
That is the real lesson here: Tc-99m is a workhorse isotope, but it rides on an infrastructure stack that is far more delicate than the routine scan it enables. A six-hour half-life leaves no place to hide, and a pipe deformation in Petten is enough to remind you that modern medicine still rests on reactors, processors, and transport schedules that have to work almost perfectly every day.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Did this article answer your question?


